Article Text

Abstract
Background: Quality control procedures vary considerably among the providers of equipment for home mechanical ventilation (HMV).
Methods: A multicentre quality control survey of HMV was performed at the home of 300 patients included in the HMV programmes of four hospitals in Barcelona. It consisted of three steps: (1) the prescribed ventilation settings, the actual settings in the ventilator control panel, and the actual performance of the ventilator measured at home were compared; (2) the different ventilator alarms were tested; and (3) the effect of differences between the prescribed settings and the actual performance of the ventilator on non-programmed readmissions of the patient was determined.
Results: Considerable differences were found between actual, set, and prescribed values of ventilator variables; these differences were similar in volume and pressure preset ventilators. The percentage of patients with a discrepancy between the prescribed and actual measured main ventilator variable (minute ventilation or inspiratory pressure) of more than 20% and 30% was 13% and 4%, respectively. The number of ventilators with built in alarms for power off, disconnection, or obstruction was 225, 280 and 157, respectively. These alarms did not work in two (0.9%), 52 (18.6%) and eight (5.1%) ventilators, respectively. The number of non-programmed hospital readmissions in the year before the study did not correlate with the index of ventilator error.
Conclusions: This study illustrates the current limitations of the quality control of HMV and suggests that improvements should be made to ensure adequate ventilator settings and correct ventilator performance and ventilator alarm operation.
- f, frequency
- HMV, home mechanical ventilation
- I/E, inspiratory/expiratory time
- Pexp, expiratory pressure
- Pins, inspiratory pressure
- V˙e, minute ventilation
- home mechanical ventilation
- quality control
- ventilator performance
- ventilator alarms
Statistics from Altmetric.com
- f, frequency
- HMV, home mechanical ventilation
- I/E, inspiratory/expiratory time
- Pexp, expiratory pressure
- Pins, inspiratory pressure
- V˙e, minute ventilation
Home mechanical ventilation (HMV) is a chronic care respiratory treatment whose application has progressively increased in the last years, as recently documented by a European survey.1 This report also showed that the quality control procedures vary considerably among the different HMV providers, probably because of the sharp increase in the number of clinical groups using HMV in the last decade and the consequent short training period.2 According to this survey, some of the procedures for the equipment follow up reported by the HMV providers suffer from inadequate quality control. In addition to the lack of standardisation of HMV quality control, there are no data on the actual performance of ventilators at home and on the potential clinical effects of ventilator dysfunction. Although HMV is generally a safe procedure,3 data from a pilot study in a limited number of patients suggested that home ventilators did not perform in accordance with their settings.4 Moreover, it has been found that ventilator settings at home may differ from the settings prescribed by the physician in charge of the patient.4
The aim of the present study was to carry out an extensive multicentre quality control survey based on testing the settings and performance of ventilators at the patient’s home. We first compared the prescribed ventilation settings, the actual settings in the ventilator control panel, and the actual performance of the ventilator measured at home. We then tested the different ventilator alarms and, finally, we ascertained whether disagreement between the prescribed settings and the actual performance of the ventilator had a major clinical impact as reflected by increased non-programmed hospital readmissions.
METHODS
The study was carried out at the homes of 300 patients (54% women) of mean (SD) age 54 (15) years selected at random from 561 patients included in the HMV programmes of the four main university hospitals in the metropolitan area of Barcelona. The random selection was constrained to maintain the proportion of patients from each hospital (44%, 33%, 17%, and 6%). The Public Health Service of Catalonia provides free HMV (ventilators, consumables, and maintenance) to all those requiring it through registered prescription hospitals and in accordance with common HMV regulations. At the time of the study HMV was supplied by four commercial companies in the Barcelona area. Ten patients were excluded from the quality control study because of technical reasons (incomplete data obtained in the home measurement procedure).
The 290 patients who participated in the study were receiving HMV for lung and airway diseases (9.5%), neuromuscular diseases (24.7%), thoracic cage abnormalities (53.0%), or hypoventilation obesity syndrome (12.8%). The duration of ventilation ranged from 1 to 16 years (52% of the patients were on home ventilation for more than 4 years). The patients were ventilated with an assist mode by means of 22 different models/versions of conventional home ventilators used in the routine HMV programmes of the participating hospitals. Volume preset ventilators were used in 153 patients and pressure preset ventilators in 137 patients; 64% of the ventilators allowed the ventilation settings in the control panel to be locked to avoid patient manipulation. Assisted ventilation was applied through a customised nasal mask (47.2%), commercially available nasal masks (46.2%), full face masks (2.3%), or a tracheostomy (4.3%). In 56.7% of the patients ventilation was applied only during the night, 40.7% of the patients were ventilated during the night plus a few hours during the day at the patient’s request, 1.3% of the patients were ventilated more than 18 hours per day, and in 1.3% of patients ventilation was applied continuously.
A specially trained nurse visited the homes of all the patients during a 4 month period. The patients were not previously informed that a ventilator check would be carried out during the nurse’s visit. The quality control protocol followed during the home visits consisted of three steps:
-
The ventilation parameters set in the control panel of the ventilator were recorded.
-
The corresponding values actually provided by the ventilator were measured by a portable system designed to test ventilators (Ventest, Soderel Medical, Heillecourt, France). The ventilator was connected to a standard resistance (5 cm H2O·s/l) – compliance (0.05 l/cm H2O) lung model (European Standards NF-EN-794-2) included in the ventilator testing system. Inspiratory and expiratory flow and pressures during the ventilator operation were recorded by a computerised unit which yielded the actual values generated by the ventilator.
-
The ventilator alarms were tested during the normal functioning of the ventilator when connected to the lung model. To test the power off alarm, the ventilator was disconnected from the mains power supply. The disconnection alarm and the obstruction alarm were tested by disconnecting the lung model from the ventilator or by completely occluding the tubing at the entrance of the lung model, respectively.
The ventilator variables analysed were minute ventilation (V˙e), frequency (f), and inspiratory/expiratory time (I/E) for volume preset ventilators (153 patients) and inspiratory (Pins) and expiratory (Pexp) pressures for pressure preset ventilators (137 patients). The differences between the ventilation variables prescribed to the patient (obtained from his/her clinical record), the values set on the ventilator panel control, and the values actually measured during the ventilator test were compared using Bland-Altman analysis.5 To define an index of ventilator error for each patient we used the data from V˙e or Pins since these can be considered to be the main variables in volume and pressure preset ventilators, respectively. The index of ventilation error was defined as the positive value of the percentage difference between the actual measured value yielded by the ventilator at home and the prescribed setting (V˙e or Pins, depending on the ventilator type). For instance, if in a pressure preset ventilator the prescribed Pins was 14 cm H2O and the measured value at home was 6 cm H2O, the index of ventilator error was 57% (57 = 100 · ABS (6–14)/14 where ABS = absolute value). ANOVA was used to ascertain whether the index of ventilator error depended on the hospital, the company that serviced the ventilator, the respiratory disease, or on the duration of ventilation (< or >4 years). The data stored in the patient clinical records were used to assess the relationship between the index of ventilator error and the number and length of non-programmed hospital readmissions in the 12 month period before the study.
This multicentre study was carried out under the auspices of the Catalan Agency for Health Technology Assessment and Research. Approval was obtained from the relevant ethics committee. The different companies involved in HMV in the metropolitan area of Barcelona were informed about the study 6 months before the start of data collection. Each participating patient was informed of the aim of the investigation by his/her attending clinical team and his/her written consent to participate was obtained.
RESULTS
Considerable differences were observed between the settings prescribed to the patient and the actual settings in the ventilator control panel, both in volume and pressure preset ventilators. Figure 1 shows the results corresponding to a representative variable in each type of ventilator (V˙e and Pins). Although the mean value of the differences was not significantly different from zero, the limits of agreement between the set and prescribed values, computed as the mean (±2SD) of the difference between variables,5 were considerable (table 1). This table also shows the wide range in the actual differences observed. These data illustrate the existence of marked discrepancies between prescribed and set values within the 5% of data which, according to the theoretical prediction, are outside the limits of agreement. As shown in table 1, similar results were found in the other ventilation variables (f, I/E and Pexp) between the settings prescribed and the actual settings in the ventilator control panel. Interestingly, the difference (in V˙e or Pins) between prescribed and set values was 4.8% (13.7%) in the ventilators which allowed the control panel settings to be locked and 8.1% (8.6%) in the ventilators where such locking was not possible. The dependence of the discrepancy between prescribed and set values on the existence of the locking option in the ventilator was significant (p = 0.046, t test).
Comparison between the ventilation values prescribed and those set on the control panel of the ventilator

Comparison between (A) minute ventilation set in the volume preset ventilator control panel and minute ventilation prescribed for the patient in 157 patients on volume preset ventilation and (B) inspiratory pressure in pressure preset ventilators in 137 patients. The differences between the two values are plotted as a function of the prescribed values. Solid lines correspond to the mean differences and dashed lines correspond to mean ±2SD (limits of agreement). In (B) the number of distinguishable symbols is lower than the number of cases because some symbols represent superimposed data from several patients.
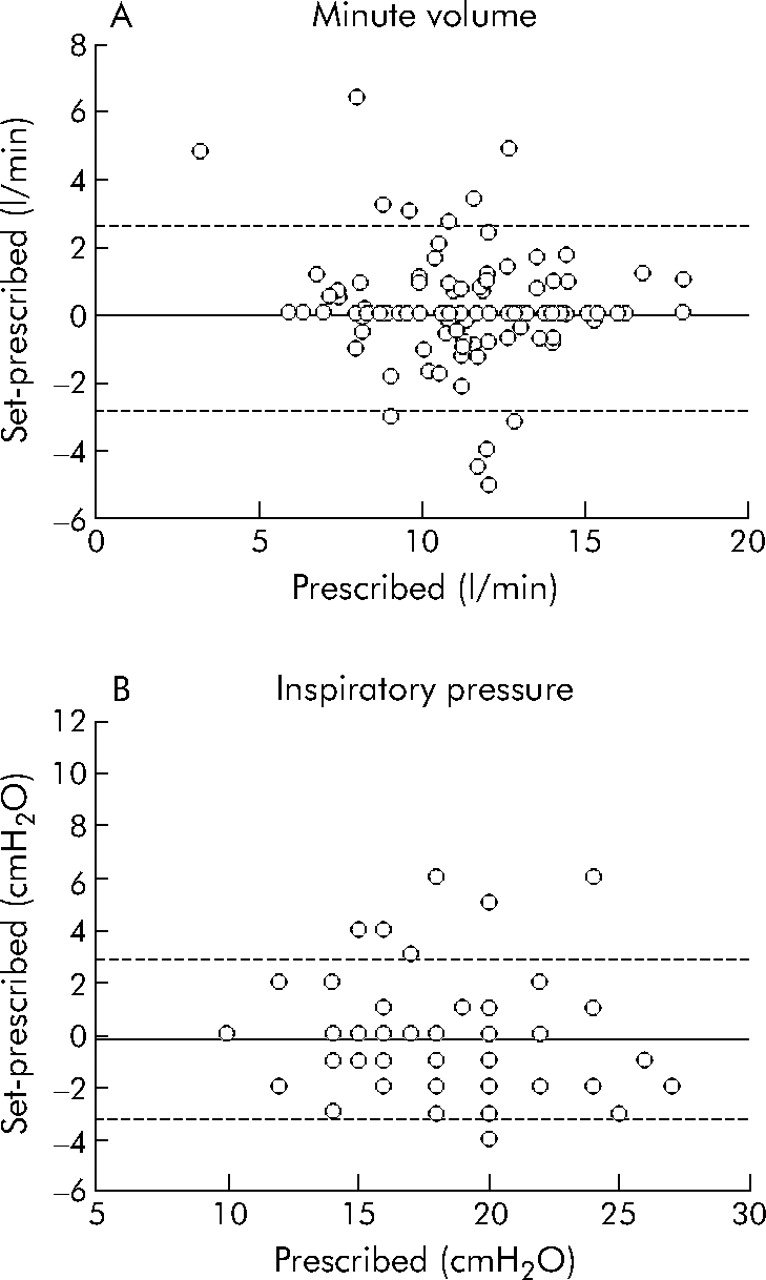
Significant differences were found between the ventilator parameters set in the control panel of the ventilator and the actual measured values. Figure 2 shows plots of the differences for V˙e and Pins, and table 2 shows the results corresponding to all the variables studied. Most of the investigated variables showed significant differences. As in table 1, the limits of agreement were wide and the range of actual differences was considerable.
Comparison between ventilator values actually measured and set on the control panel of the ventilator

Comparison between (A) actual generated minute ventilation and minute ventilation set in the volume preset ventilator control panel for the 157 patients on volume preset ventilation and (B) actual generated inspiratory pressure and inspiratory set pressure in pressure preset ventilators for the 137 patients on pressure preset ventilation. The differences between the two values in each case are plotted as a function of the set values. Solid lines correspond to the mean differences in each plot and dashed lines correspond to mean ±2SD (limits of agreement). In (B) the number of distinguishable symbols is lower than the number of cases because some symbols represent superimposed data from several patients.
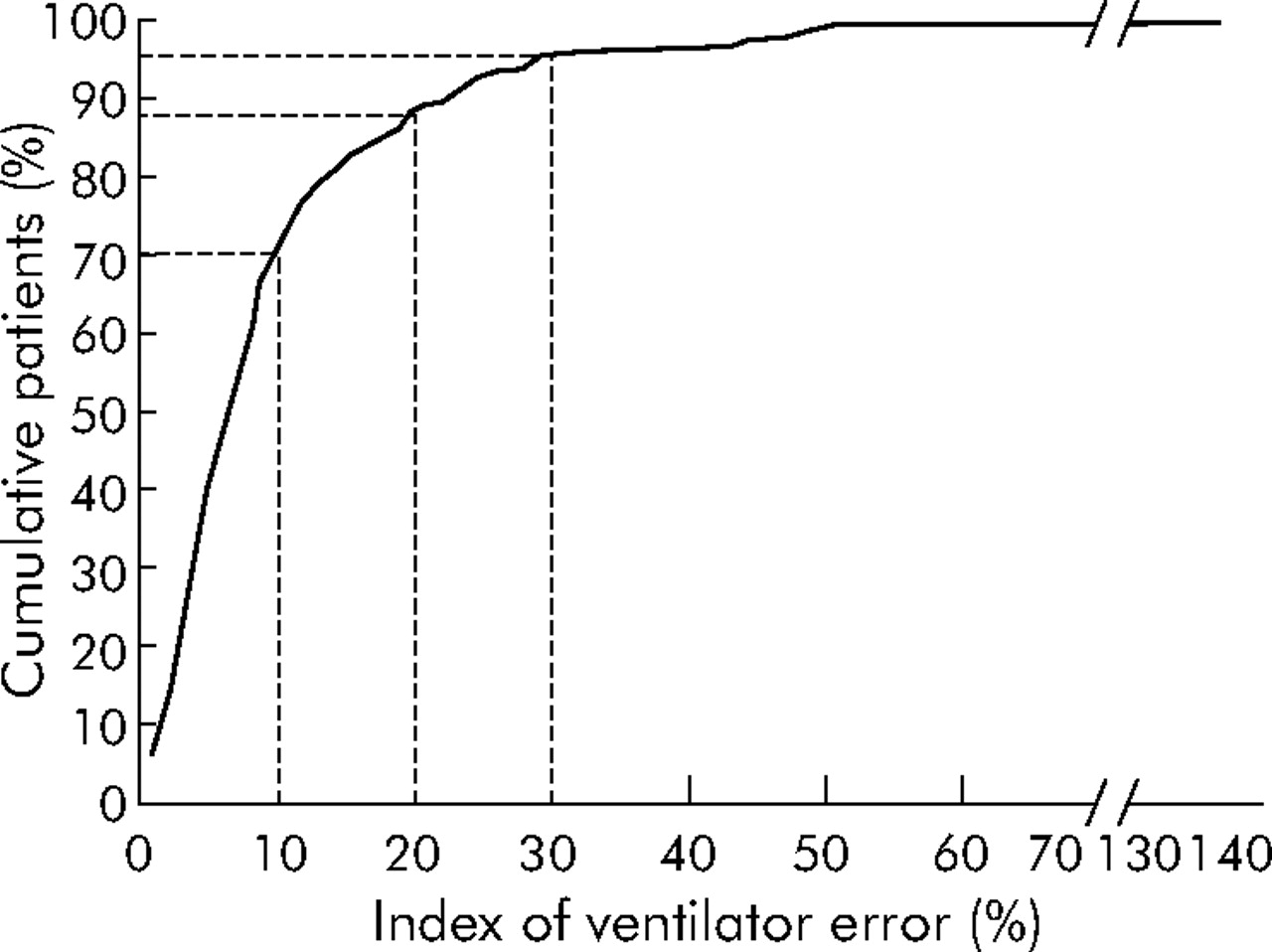
The index of ventilator error (computed as defined in the Methods section) was similar in volume and pressure preset ventilators: 9.6% (13.2%) (range 0–133%) and 10.5% (11.7%) (range 0–54%), respectively. Figure 3 shows the cumulative percentage of all patients as a function of the index of error of his/her ventilator. In 70% of patients the index of ventilator error was lower than 10%. The percentage of patients with an index of ventilator error exceeding 20% was 13%. The index of ventilator error exceeded 30% in 4% of patients. The ventilator error index did not significantly depend on the hospital, the company that serviced the ventilator, or on the respiratory disease of the patient (p>0.05). The index of ventilator error was significantly greater for patients on HMV for a period exceeding 4 years (11.6%) than for those receiving the treatment for a shorter time (8.4%; p = 0.036).
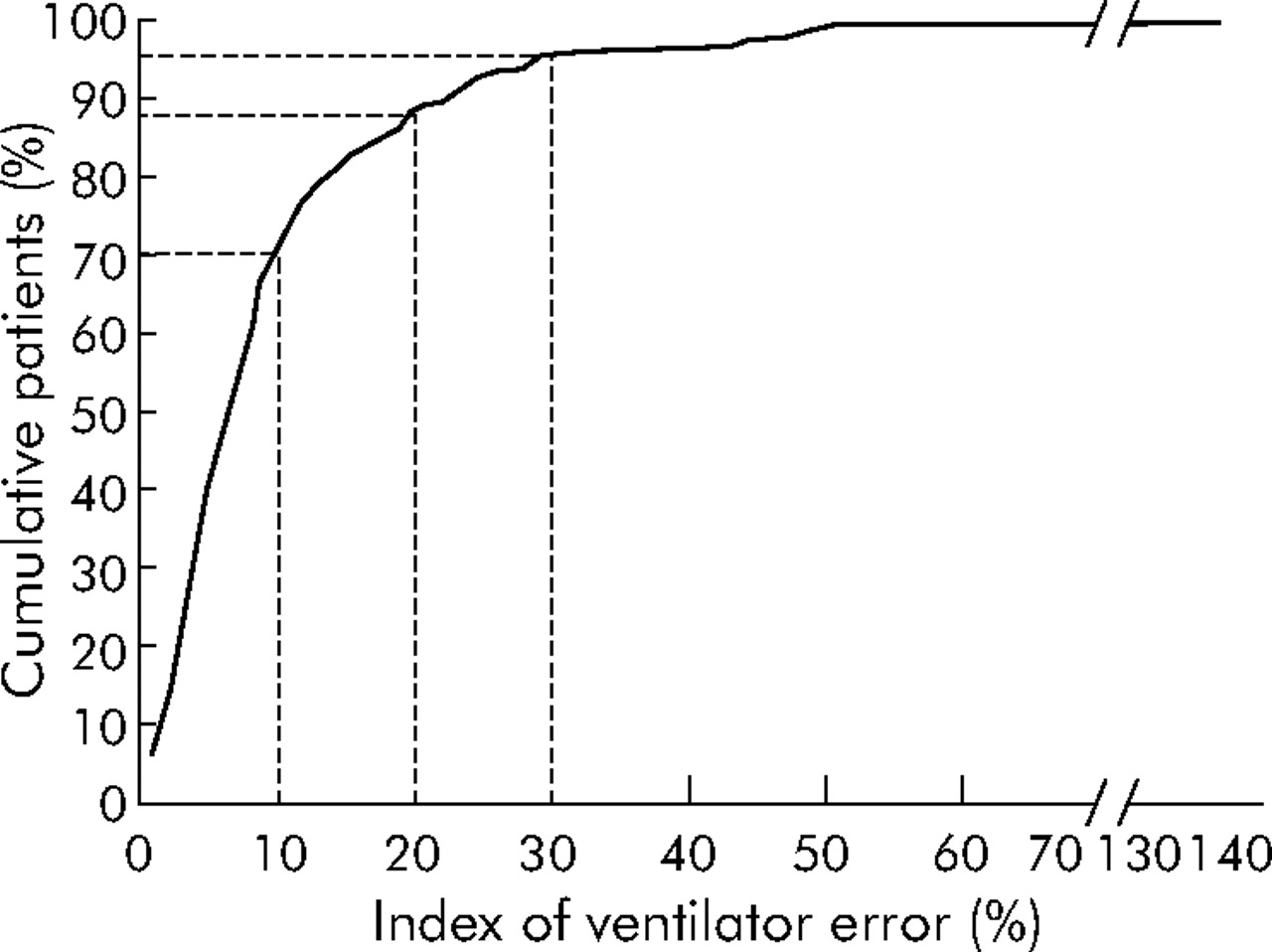
Cumulative percentage of patients as a function of the index of error of his/her ventilator. The ventilator error was assessed as error in minute ventilation or in inspiratory pressure for volume and pressure preset ventilators, respectively.
The number of ventilators with built in alarms for power off, disconnection, or obstruction was 225, 280 and 157, respectively. These alarms did not work in two (0.9%), 52 (18.6%), and eight (5.1%) ventilators, respectively. All the alarms worked correctly in the patients subjected to 24 hour ventilation.
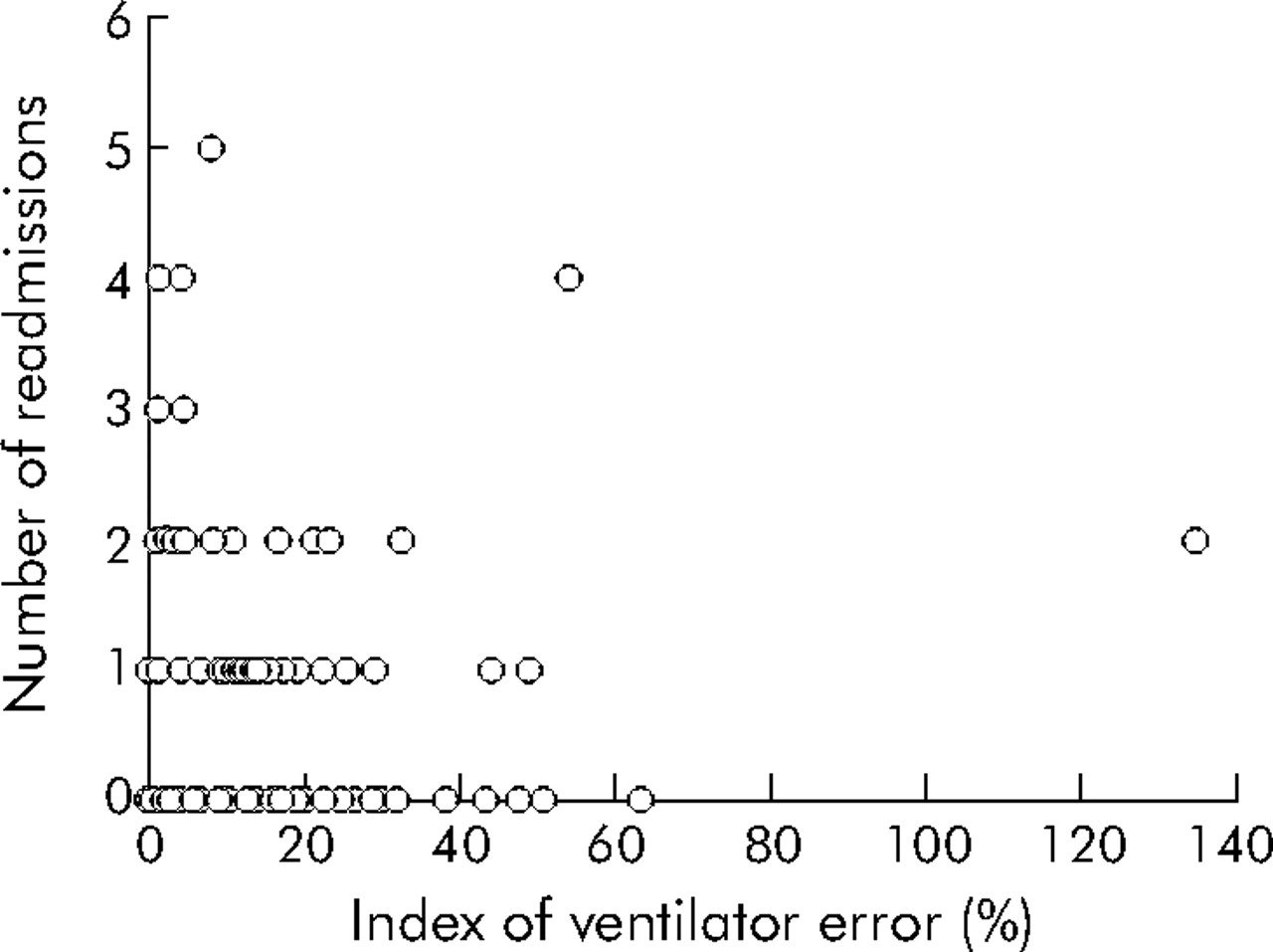
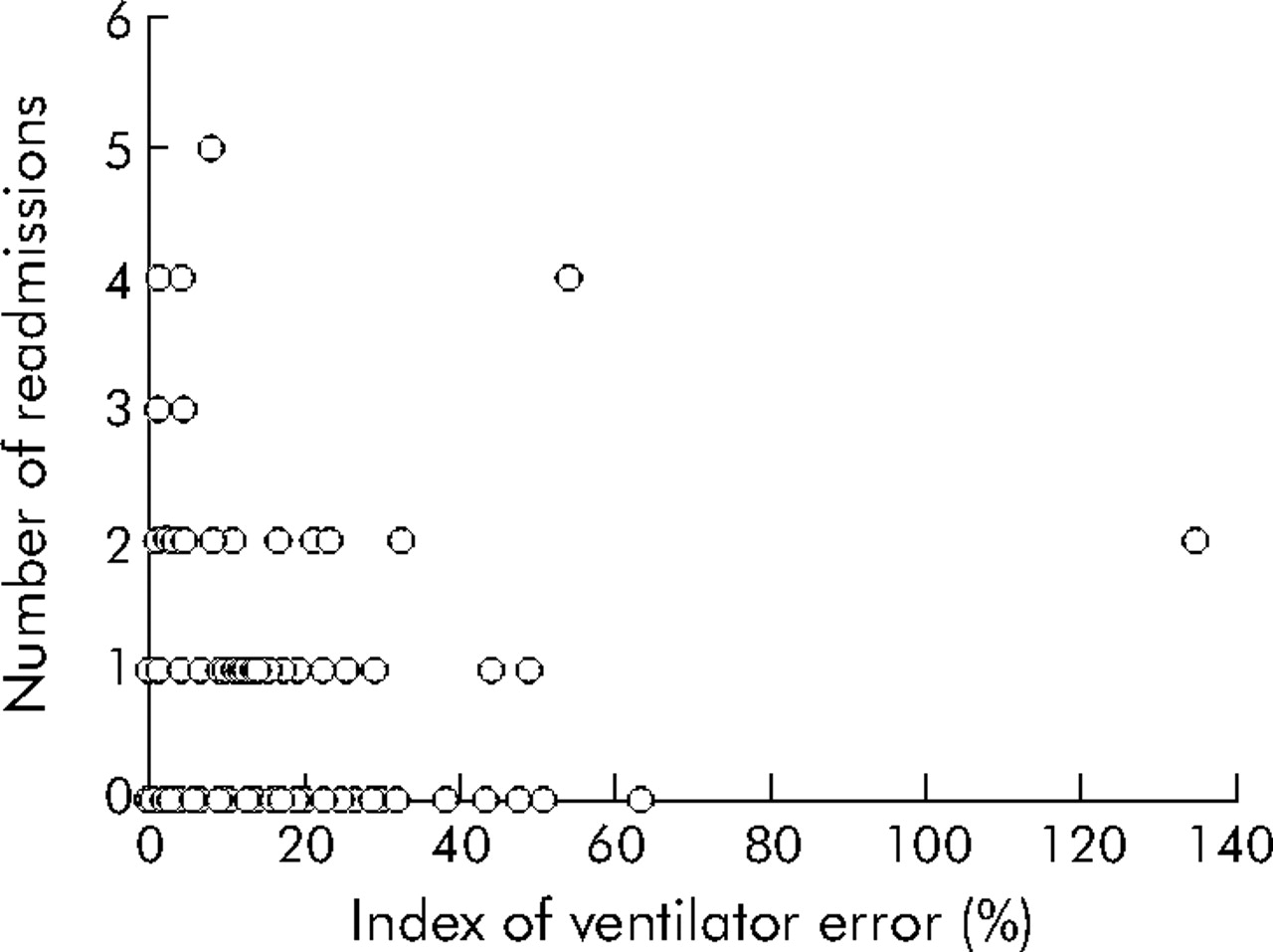
The number of non-programmed hospital readmissions in the last year before the study did not correlate with the index of ventilator error (fig 4). A similar result was found when the number of total days of non-programmed readmission was compared with the ventilator error index.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between the number of non-programmed hospital readmissions in the previous year and the index of error of the home ventilator.
DISCUSSION
In this study of the settings and performance of mechanical ventilators at the patient’s home, we observed considerable differences between the settings prescribed, the values set at the control panel of the ventilator, and the ventilation values effectively yielded by the equipment. We also found underperformance in the ventilator alarms. As the errors in the ventilators did not depend on the hospital or on the company servicing the equipment, the deficiencies observed must be attributed to limitations of the quality control procedure followed at the centres studied. The fact that the index of ventilator error was greater in the patients in whom HMV started earlier is consistent with poor quality control. Indeed, the probability that the ventilator settings were changed in an uncontrolled way and that their clinical records were not adequately updated is increased in these patients. Given that the quality control of equipment at the centres included in this study was similar to the average in Europe,2 the results found in the present study may be regarded as representative.
To the best of our knowledge, this is the first extensive multicentre study to test the actual performance of normally operating ventilators at the patient’s home. An earlier study on ventilator dysfunction covering a wide patient population was retrospectively based on a register of incidents and, hence, the results did not come from the inspection of ventilators at homes randomly selected from the general HMV population.3
During the ventilator home test we recorded the parameter settings on the ventilator control panel and measured the actual ventilation provided by the device. Since home visits require a portable system, the standardised lung model used was passive. Data such as ventilator triggers which might also affect patient comfort and compliance were therefore not tested. However, given that we found similar results in all the parameters studied, the settings involved in the active response of the ventilator could be affected by the same level of deficiencies.
One interesting finding from this study was that the parameter values set in the control panel of the ventilator did not coincide with the settings prescribed to the patient (fig 1 and table 1). Such a difference, which cannot be attributed to equipment malfunction, could be due to the fact that changes in setting prescription during the HMV follow up had not been adequately registered in the patient’s clinical record or to the fact that the patient had (in)voluntarily modified the ventilator settings. Although manipulation of the control panel by the patient is not possible in modern ventilators, a non-negligible number of ventilators in current use still allow an easy modification of the settings. The fact that the patient modifies the ventilator settings is not necessarily detrimental. In some cases it is possible that the patient adapts the ventilator settings to improve his/her comfort. In fact, it should be borne in mind that, while the setting titration is carried out at patient discharge, the pathophysiological status of the patient evolves with the result that some months after discharge the ventilation that the patient needs is not the same as the one titrated at discharge. It is also possible that the patient adapts the settings to counterbalance the unintentional leak level from the mask which can change as the patient rearranges the mask to improve comfort. Accordingly, this action could be interpreted positively as a sign of patient empowerment. However, in some cases the patient could wrongly modify the ventilator settings with the result that the beneficial effects of the treatment are reduced. In any case, the fact that the patient is ventilated with settings that are different from the ones prescribed to him/her should be regarded as a quality control deficiency. Indeed, to adequately monitor the normal clinical evolution of the patient and to interpret potential acute incidents, the physician in charge of the patient follow up must be aware of how the patient is actually ventilated.
Another finding of this study was that the ventilators did not perform in agreement with the settings in the control panel (fig 2 and table 2). Specifically, the minute ventilation provided by the device progressively worsened as the set value increased. The fact that home ventilators tended to underperform when subjected to high level requirements has already been documented.6 However, recent data indicate that the performance of modern ventilators has improved.7 To interpret the importance of the results reported in fig 2 and table 2 adequately, it should be stressed that the lung model used in the home test featured the resistance and elastance of a normal respiratory system. According to the literature, greater underperformance is expected if a lung model with high resistance/elastance mimicking patients with increased impedance is used.6 The fact that the normal servicing of the ventilators did not detect the observed underperformance indicates that the quality control carried out by the companies could be improved.
In this study we also focused on ventilator alarms. A significant proportion of the ventilators did not incorporate alarms. Moreover, the alarms did not work when subjected to an effective test in a non-negligible number of ventilators with built in alarms because these were not activated or because they failed. Although the alarms operated correctly in all the patients subjected to 24 hour ventilation, our results highlight the problem of quality control—namely, the question of adapting the alarms to the needs of different patients. It seems reasonable that, if the ventilator is equipped with an alarm, it should be activated and should work properly even if the patient is not fully dependent on the ventilator.
Although the results found in this study could raise significant concerns about the quality control of home ventilators, it should be noted that the equipment dysfunctions detected were not correlated with major indices of treatment failure such as non-programmed readmissions. However, we did not ascertain whether ventilator malfunction could affect other parameters such as patient compliance, tolerance, side effects, or quality of life. Although all the patients remained stable while receiving HMV, it is possible that improving the HMV performance could in some cases enhance patient comfort, treatment compliance, and clinical effectiveness.8 The finding that safe and effective treatment is compatible with some ventilator errors could be attributed to the fact that, in most patients subjected to HMV, the required “dose” of treatment is not critical in terms of patient comfort and physiological effects.9,10 According to this interpretation, most stable patients on HMV need ventilatory support, but the amount of support to ensure adequate treatment of the patient falls within a relatively wide range of settings.9,10 The question of whether the HMV settings should be titrated in terms of patient comfort or physiological improvement remains open to debate.11,12
In conclusion, this study illustrates the current limitations of the quality control of HMV in a representative clinical context. The results suggest that HMV quality control can be upgraded to ensure adequate ventilator settings, correct ventilator performance, and ventilator alarms operation. In addition to reducing the risk of possible accidents, improved HMV quality control will provide the patient with ventilatory support closer to that prescribed and will reassure both the patient and the physician about the adequacy of the treatment.
Acknowledgments
The authors thank Isabel Rubio for performing the nurse home visits and Dr J V Pons, director of the Catalan Agency for Health Technology Assessment and Research, for organising the study. The authors acknowledge Soderel Medical (Heillecourt, France) for kindly lending the Ventest system to carry out the study.
REFERENCES
Footnotes
-
Published Online First 7 February 2006
-
This work was supported in part by grants from Ministerio de Ciencia y Tecnologia (SAF 2002-03616 and SAF 2003-01334), Ministerio de Sanidad y Consumo (Red GIRA-G03/063 and Red RESPIRA-C03/11, FIS-PI040929) and SEPAR. The companies Airliquide SL, Oxigen Salud SA, Oximesa SL, and ResMed Spain SL partially supported this study through donations to the Catalan Agency for Health Technology Assessment and Research.
-
Competing interests: none declared.
Linked Articles
- Airwaves