Article Text

Statistics from Altmetric.com
Summary of recommendations and good practice points
How should the diagnosis of bronchiectasis be determined?
Recommendations – Imaging
Perform baseline chest X-ray in patients with suspected bronchiectasis. (D)
Perform a thin section computed tomography scan (CT) to confirm a diagnosis of bronchiectasis when clinically suspected. (C)
Perform baseline imaging during clinically stable disease as this is optimal for diagnostic and serial comparison purposes. (D)
Good practice points
CT imaging protocol
The most appropriate imaging protocol will vary according to scanner technology and patient factors.
When using volumetric CT, dose reduction techniques including adaptive mA and kV and iterative reconstruction should be utilised where available.
Typical CT imaging parameters for the diagnosis of bronchiectasis are:
Slice thickness: ≤1mm
Reconstruction algorithm: – high spatial frequency
kVp: 100-140
mAs (or effective mAs): 100 – 200
Gantry rotation time: <0.5s
CT features of bronchiectasis
Bronchiectasis is defined by bronchial dilatation as suggested by one or more of the following:
Bronchoarterial ratio >1 (internal airway lumen vs adjacent pulmonary artery)
Lack of tapering
Airway visibility within 1cm of costal pleural surface or touching mediastinal pleura.
The following indirect signs are commonly associated with bronchiectasis:
Bronchial wall thickening
Mucus impaction
Mosaic perfusion / air trapping on expiratory CT
General
CT scanning can also aid in identifying an aetiology of bronchiectasis eg Allergic bronchopulmonary aspergillosis (ABPA), Non-tuberculous mycobacteria (NTM), primary ciliary dyskinesia, alpha one antitrypsin deficiency, Williams Campbell syndrome and a foreign body.
In whom should the diagnosis of bronchiectasis be suspected?
Recommendations
Consider investigation for bronchiectasis in patients with persistent production of mucopurulent or purulent sputum particularly with relevant associated risk factors. (D)
Consider investigation for bronchiectasis in patients with rheumatoid arthritis if they have symptoms of chronic productive cough or recurrent chest infections. (C)
Consider investigation for bronchiectasis in patients with Chronic Obstructive Pulmonary Disease (COPD) with frequent exacerbations (two or more annually) and a previous positive sputum culture for P. aeruginosa whilst stable. (B)
Consider investigation for bronchiectasis in patients with inflammatory bowel disease and chronic productive cough. (C)
Good practice points
In at risk groups, if bronchiectasis is suspected, bronchiectasis needs confirmation.
In patients with COPD, investigation for bronchiectasis may be appropriate especially in the presence of chronic productive cough with positive sputum cultures for potentially pathogenic microorganisms (PPM) whilst stable or 2 or more exacerbations in the preceding 12 months.
In patients with asthma, investigation for bronchiectasis may be appropriate with severe or poorly-controlled disease.
In patients with a history of HIV-1 infection, solid organ and bone marrow transplant, and history of immunosuppressive therapy for lymphoma and vasculitis, investigation for bronchiectasis may be appropriate with symptoms of chronic productive cough or recurrent chest infections.
In patients with chronic rhinosinusitis, investigation for bronchiectasis may be appropriate with symptoms of chronic productive cough or recurrent chest infections.
In patients with other connective tissue disease or inflammatory bowel disease, investigation for bronchiectasis may be appropriate if they have symptoms such as chronic productive cough or recurrent chest infections.
Investigation for bronchiectasis may be appropriate in otherwise healthy individuals with a cough that persists for longer than 8 weeks, especially with sputum production or a history of an appropriate trigger (see BTS Recommendations for the management of cough in adults (61)).
Investigations for causes of bronchiectasis
Recommendations (see Table 1)
A panel of investigations should be performed to establish the underlying cause of bronchiectasis. (B)
Co-morbidities and past medical history should be recorded in patients diagnosed with bronchiectasis to identify relevant and possibly causative disease such as rheumatoid arthritis, COPD, asthma, gastro-oesophageal reflux disease and inflammatory bowel disease. (C)
Measure full blood count, serum total IgE and assessment of sensitisation (specific IgE or skin prick test) to Aspergillus fumigatus in all patients with bronchiectasis. (D)
Serum Immunoglobulin G (IgG), Immunoglobulin A (IgA) and Immunoglobulin M (IgM) should be performed in all patients with bronchiectasis. (C)
Consider measuring baseline specific antibody levels against capsular polysaccharides of Streptococcus pneumoniae in all patients to investigate for specific antibody deficiency. If pneumococcal antibodies are low, immunise with 23 valent polysaccharide pneumococcal vaccine, followed by measurement of specific antibody levels 4–8 weeks later. (D)
Test for cystic fibrosis (according to NICE Guidelines for Cystic Fibrosis (CF)) in patients with supporting clinical features, for example, early onset, male infertility, malabsorption, pancreatitis. (B)
Test for Primary Ciliary Dyskinesia (PCD) (according to ERS Guidelines for PCD Diagnosis) in patients with supporting clinical features, including a history of neonatal distress, symptoms from childhood, recurrent otitis media, rhinosinusitis, or infertility. (A)
Sputum cultures should be performed in all patients with bronchiectasis for routine and mycobacterial culture. (D)
Quick summary guide
Good practice points
A previous diagnosis of idiopathic bronchiectasis should prompt careful reinvestigation for a primary cause in the context of a deteriorating clinical course or a young patient (usually considered to be age 50 and under but not limited to this age group).
Referral to a specialist centre for investigation should be considered for young patients (usually considered to be age 50 and under but not limited to this age group) and those with apparent idiopathic bronchiectasis especially where there is evidence of progressive disease.
Consider testing for rheumatoid factor (RF), anti-cyclic citrullinated peptide (anti CCP), antinuclear antibodies (ANA) and anti-neutrophil cytoplasmic antibodies (ANCA) in patients with coexisting clinical features of arthritis, connective tissue disease and/or systemic vasculitis.
Consider testing for alpha 1 antitrypsin (A1AT) deficiency in patients with coexisting basal panacinar emphysema.
Investigations for reflux and aspiration should be undertaken only in symptomatic patients, or where there are other suggestive clinical features.
Consider bronchoscopy for patients with localised disease to rule out an endobronchial lesion or foreign body as the cause of bronchiectasis.
A bronchial aspiration or bronchial wash targeting the areas of bronchiectasis from CT scan of the chest should be considered in patients who do not expectorate and can be particularly helpful in the diagnosis of NTM pulmonary disease.
Serum protein electrophoresis should be performed in all patients with bronchiectasis with raised immunoglobulins.
Consider HIV-1 serology in patient with bronchiectasis depending on prevalence of HIV-1 and clinical features suggestive of increased risk of retroviral infection.
Research recommendations
Consensus criteria for diagnosis of ABPA need to be validated in bronchiectasis cohorts.
Consensus criteria for definition of abnormal post pneumococcal test immunisation antibody responses need to be validated in bronchiectasis cohorts.
Severity scoring
Good practice point
Consider using the bronchiectasis severity index which may help guide management.
Stable state treatment
Which patients should be taught airway clearance techniques?
Recommendation
Teach individuals with bronchiectasis to perform airway clearance. (D)
Good practice points
Airway clearance techniques should be taught by a respiratory physiotherapist.
At initial assessment, a respiratory physiotherapist should educate the patient about their condition and if appropriate give advice on adjuncts (inhaled/oral therapy or exercise) that may enhance effectiveness of their chosen airway clearance technique.
Patients admitted with an exacerbation of bronchiectasis should be seen daily by a respiratory physiotherapist until their airway clearance is optimised.
Which airway clearance techniques should be taught?
Recommendations
Offer active cycle of breathing techniques or oscillating positive expiratory pressure to individuals with bronchiectasis. (D)
Consider gravity assisted positioning (where not contraindicated) to enhance the effectiveness of an airway clearance technique. (D)
Good practice points
CT imaging should be reviewed to complement the physiotherapy assessment. Where indicated, this information could be used in order to teach the patient the appropriate postural drainage position(s) for their affected bronchopulmonary segment(s).
Patients should be made aware of the range of available airway clearance techniques.
Consider patient preference and adherence when recommending an airway clearance technique.
Consider the inclusion of the forced expiration technique (huff) should be considered for all airway clearance techniques.
Consider modified postural drainage (no head down tilt) in patients for whom postural drainage is contraindicated or not tolerated.
If symptoms of gastroesophageal reflux increase with modified postural drainage (no head down tilt), an airway clearance technique in the sitting position should be taught.
Consider autogenic drainage, positive expiratory pressure, high frequency chest wall oscillation and intrapulmonary percussive ventilation as an alternative airway clearance technique if other techniques are not effective or acceptable to the patient.
Patients should be encouraged to perform regular physical exercise (plus the forced expiration technique/huff) to promote airway clearance.
If there is ongoing haemoptysis, refer back to the respiratory physiotherapist to determine the optimum airways clearance technique.
Airway clearance techniques during an acute exacerbation
Good practice points
Manual techniques may be offered to enhance sputum clearance when the patient is fatigued or undergoing an exacerbation.
Consider intermittent positive pressure breathing or non-invasive ventilation during an acute exacerbation to offload the work of breathing so fatigued and/or breathless patients can tolerate a longer treatment session and can adopt postural drainage positions.
Research recommendations
Randomised controlled trials using clinically important outcome measures are required to assess the effectiveness of airway clearance techniques in varying severities of bronchiectasis.
Randomised controlled trials are required to evaluate the effects of airway clearance techniques in patients who are undergoing an exacerbation.
How often should patients carry out airway clearance techniques?
Good practice points
The frequency and duration of the airway clearance technique should be tailored to the individual and may alter during periods of exacerbation.
Advise individuals to perform their airway clearance technique for a minimum of 10 minutes (up to a maximum of 30 minutes). After this time they should continue until two clear huffs or coughs are completed, or until the patient is starting to become fatigued.
How soon should the patient be reviewed after the initial assessment?
Good practice points
Individuals that have been assessed and taught an airway clearance technique should be reviewed by a respiratory physiotherapist within 3 months of their initial assessment.
Individuals with bronchiectasis who are followed up in secondary care should be assessed by a respiratory physiotherapist as part of their annual clinical review to ensure their airway clearance regimen is optimised.
All individuals with a deterioration in their condition (increased frequency of exacerbations and/or worsening of symptoms) should have their airway clearance technique reviewed by a respiratory physiotherapist (See figure 1 – management of the deteriorating patient).

Management of the deteriorating patient.
Mucoactives in bronchiectasis
Recommendations
Do not routinely use recombinant human DNase in adults with bronchiectasis. (A)
Consider the use of humidification with sterile water or normal saline to facilitate airway clearance. (D)
Good practice points
Consider a trial of mucoactive treatment in patients with bronchiectasis who have difficulty in sputum expectoration.
Perform an airway reactivity challenge test when inhaled mucoactive treatment is first administered.
Consider pre-treatment with a bronchodilator prior to inhaled or nebulised mucoactive treatments especially in individuals where bronchoconstriction is likely (patients with asthma or bronchial hyper-reactivity and those with severe airflow obstruction FEV1<1 litre).
If carbocysteine is prescribed, a 6 month trial should be given and continued if there is ongoing clinical benefit.
See Figures 3 and 4 and Appendix 2.
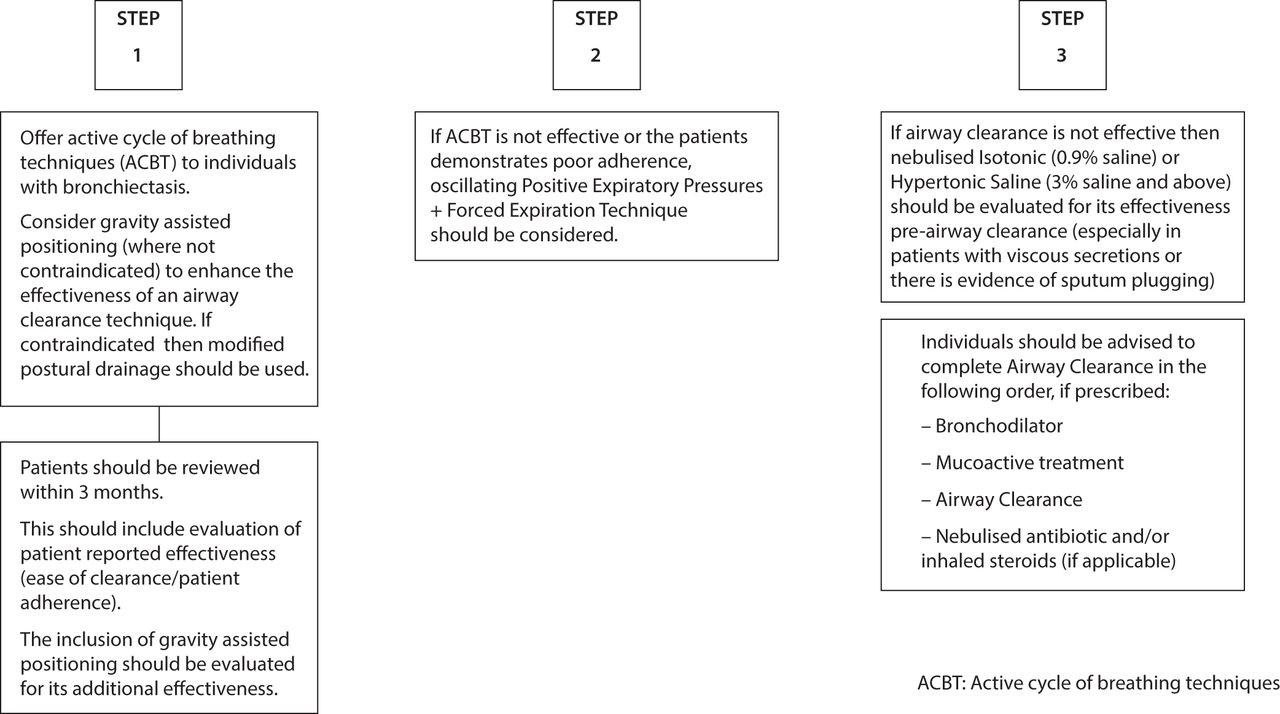
Physiotherapy management-stepwise airway clearance.

Airway clearance - exacerbations.
Appendix 2
Research recommendation
Randomised controlled trials are needed to assess the long term impact of muco-active therapies.
What is the evidence for long term anti-inflammatory therapies in bronchiectasis?
Recommendations
Do not routinely offer inhaled corticosteroids to patients with bronchiectasis without other indications (such as ABPA, chronic asthma, COPD and inflammatory bowel disease). (B)
Do not offer long-term oral corticosteroids for patients with bronchiectasis without other indications (such as ABPA, chronic asthma, COPD, inflammatory bowel disease). (D)
Do not routinely offer phosphodiesterase type 4 (PDE4) inhibitors, methylxanthines or leukotriene receptor antagonists for bronchiectasis treatment. (D)
Do not routinely offer CXCR2 antagonists, neutrophil elastase inhibitors or statins for bronchiectasis treatment. (B)
Good practice point
Inhaled corticosteroids have an established role in the management of asthma and in a proportion of patients with COPD which are common co-morbid conditions in bronchiectasis.
Research recommendation
Randomised controlled trials are needed to assess the long term impact of anti-inflammatory therapies.
What treatments improve outcomes for patients with stable bronchiectasis? (see Figure 2 and Appendix 2 and 3)

Stepwise management.
Appendix 3
Recommendations
Consider long term antibiotics in patients with bronchiectasis who experience 3 or more exacerbations per year. (A)
In these patients, the following are recommended
P. aeruginosa colonised patients
Use inhaled colistin for patients with bronchiectasis and chronic Pseudomonas aeruginosa infection. (B)
Consider inhaled gentamicin as a second line alternative to colistin for patients with bronchiectasis and chronic P. aeruginosa infection. (B)
Consider azithromycin or erythromycin as an alternative (eg, if a patient does not tolerate inhaled antibiotics) to an inhaled antibiotic for patients with bronchiectasis and chronic P. aeruginosa infection. (B)
Consider azithromycin or erythromycin as an additive treatment to an inhaled antibiotic for patients with bronchiectasis and chronic P. aeruginosa infection who have a high exacerbation frequency. (D)
Non- P. aeruginosa colonised patients
e. Use azithromycin or erythromycin for patient with bronchiectasis. (A)
f. Consider inhaled gentamicin as a second line alternative to azithromycin or erythromycin. (B)
g. Consider doxycycline as an alternative in patients intolerant of macrolides or in whom they are ineffective. (C)
Good practice points
Antimicrobial stewardship is important
Prior to starting long term macrolides, for safety reasons: (1) ensure no active NTM infection with at least one negative respiratory NTM culture; (2) use with caution if the patient has significant hearing loss needing hearing aids or significant balance issues.
Prior to starting long term inhaled aminoglycosides, for safety reasons: (1) avoid using if creatinine clearance <30ml/min; (2) use with caution if the patient has significant hearing loss needing hearing aids or significant balance issues; (3) avoid concomitant nephrotoxic medications.
Counsel patients about potential major side effects with long term antibiotics, and to seek urgent attention if these develop.
Review the patient’s culture and mycobacterial status, optimise airway clearance and treat other associated conditions before starting long term antibiotics.
Prophylactic antibiotics should be only started by respiratory specialists.
Review patients on long term antibiotics six monthly with assessment of efficacy, toxicity and continuing need. Monitor sputum culture and sensitivity regularly, although in vitro resistance may not affect clinical efficacy.
As adverse event frequency of azithromycin is likely to be dose related, 250mg 3 x /week is a pragmatic starting dose which can then be increased according to clinical response and adverse events.
Thresholds for long term treatment may reduce if the patient is symptomatic between exacerbations and/or the exacerbations respond poorly to treatment and/or the patient is at high risk of severe exacerbation for example, immunosuppressed.
Long term antibiotic choice is complex and has to take into account factors such as tolerance, allergies and sensitivity, therefore in some circumstances, other long term antibiotic regimens may be appropriate (see appendix 3).
Perform a suitable challenge test when stable before starting inhaled antibiotics (see appendix 2)
Consider cyclical IV antibiotics in patients with repeated infections (≥5/year) despite other treatments.
Alternative inhaled/nebulised agents may become licensed as international studies are completed.
For patients receiving long term prophylactic oral antibiotics, the preferred option is to remain on the same antibiotic as opposed to monthly rotation of antibiotics. If there is a subsequent lack of efficacy, the antibiotic can be changed guided by sensitivity results.
Research recommendation
Long term randomised controlled trials of oral and inhaled antibiotics are needed to assess their efficacy and safety in patients with bronchiectasis who have frequent respiratory tract infections with recurrent P. aeruginosa infection or other potential pathogenic micro-organisms.
Does long term bronchodilator treatment improve outcomes for patients with bronchiectasis?
Recommendations
Use of bronchodilators in patients with bronchiectasis and co-existing COPD or asthma should follow the guideline recommendations for COPD or asthma. (D)
Offer a trial of long acting bronchodilator therapy in patients with symptoms of significant breathlessness. (D)
Reversibility testing to beta 2 agonist or anticholinergic bronchodilators may help to identify patients with co-existing asthma but there is no evidence to suggest that a response is required in order to benefit from bronchodilators. (D)
Pulmonary rehabilitation
Recommendations
Offer pulmonary rehabilitation to individuals who are functionally limited by shortness of breath (Modified Medical Research Council (MMRC) Dyspnoea Scale ≥ 1). (B)
Consider the use of inspiratory muscle training in conjunction with conventional pulmonary rehabilitation to enhance the maintenance of the training effect. (B)
Good practice points
Educate all individuals with bronchiectasis on the importance of an exercise training programme.
Consider the 6 minute walk test (MWT) and/or the incremental shuttle walking test (ISWT) when evaluating exercise capacity pre/post pulmonary rehabilitation in bronchiectasis. Prior to this, practice tests should be carried out to eliminate any learning effect.
Pulmonary rehabilitation providers should offer education sessions tailored to the needs of individuals with bronchiectasis (e.g. airway clearance techniques, the pathophysiology of bronchiectasis and relevant inhaled therapy).
Pulmonary rehabilitation exercise and education sessions should be provided by appropriately qualified health care practitioners.
Further information on Pulmonary rehabilitation is provided in the BTS Quality Standards for Pulmonary Rehabilitation (https://www.brit-thoracic.org.uk/standards-of-care/quality-standards/bts-pulmonary-rehabilitation-quality-standards/)
Research recommendations
The role of education, self management plans and who delivers the pulmonary rehabilitation needs to be explored.
The role of pulmonary rehabilitation after exacerbations requiring hospital admission needs to be explored.
The incidence of cross-infection of respiratory pathogens in the group exercise setting should be investigated in the bronchiectasis population.
What is the role of surgery in managing bronchiectasis?
Recommendations
Consider lung resection in patients with localised disease whose symptoms are not controlled by medical treatment optimised by a bronchiectasis specialist. (D)
Offer multidisciplinary assessment, including a bronchiectasis physician, a thoracic surgeon and an experienced anaesthetist, of suitability for surgery and pre-operative assessment of cardiopulmonary reserve post resection. (D)
Good practice point
Consider nutritional support and pre-operative pulmonary rehabilitation before surgical referral.
Lung transplantation for bronchiectasis
Recommendations
Consider transplant referral in bronchiectasis patients aged 65 years or less if the FEV1 is <30% with significant clinical instability or if there is a rapid progressive respiratory deterioration despite optimal medical management. (D)
Consider earlier transplant referral in bronchiectasis patients with poor lung function and the following additional factors: massive haemoptysis, severe secondary pulmonary hypertension, ICU admissions or respiratory failure (particularly if requiring NIV).(D)
Good practice points
Discuss appropriate patients with a transplant centre prior to formal referral.
Optimise management of comorbidities such as osteoporosis and maintain physical condition through pulmonary rehabilitation prior to transplant.
What is the role of influenza and pneumococcal vaccination in management of bronchiectasis
Recommendations
Offer annual influenza immunisation to all patients with bronchiectasis. (D)
Offer polysaccharide pneumococcal vaccination to all patients with bronchiectasis. (D)
Good practice point
Consider influenza vaccination in household contacts of patients with immune deficiency and bronchiectasis to reduce the risks of secondary transmission.
Consider use of 13 valent protein conjugate pneumococcal vaccine in patients with bronchiectasis who do not have an appropriate serological response to standard polysaccharide vaccine (23 valent carbohydrate Pneumococcal vaccine).
Treatment of respiratory failure
Recommendations
Consider long term oxygen therapy for patients with bronchiectasis and respiratory failure, using the same eligibility criteria as for COPD. (D)
Consider domiciliary non-invasive ventilation with humidification for patients with bronchiectasis and respiratory failure associated with hypercapnia, especially where this is associated with symptoms or recurrent hospitalisation. (D)
Bronchiectasis and other treatments
Recommendation
Do not routinely recommend alternative treatments (for example cough suppression, nutritional supplementation, complementary therapy/homeopathy, supplemental treatments) as part of the management of patients with bronchiectasis. (D)
Good practice point
Record patient’s weight and BMI at each clinic appointment.
Research recommendations
Further interventional/randomised controlled trials needed to establish the role of any alternative therapies in the management of bronchiectasis.
Studies assessing the benefits of nutritional supplementation in patients with bronchiectasis should be undertaken.
Do pathogens have an impact on prognosis in bronchiectasis?
Recommendations
Consider patients with chronic P. aeruginosa colonisation at higher risk of bronchiectasis-related complications. (B)
Perform regular sputum microbiology screening for patients with clinically significant bronchiectasis to monitor for pathogens and detect new isolation of P. aeruginosa. (C)
What is the evidence for the role of viruses/fungal disease in patients with bronchiectasis?
Good practice points
Testing to detect viral infection should be considered in patients with an exacerbation of bronchiectasis.
Do not routinely use anti-fungal therapy without evidence of fungal disease. Fungal cultures can be positive on those receiving long-term antibiotic therapy.
Does eradication of potentially pathogenic microorganisms improve outcomes in patients with stable bronchiectasis?
Recommendations
Offer patients with bronchiectasis associated with clinical deterioration and a new growth of P. aeruginosa (1st isolation or regrowth in the context of intermittently positive cultures) eradication antibiotic treatment. (first line treatment: ciprofloxacin 500–750 mg bd for 2 weeks; second line treatment: iv antipseudomonal beta-lactam ± an iv aminoglycoside for 2 weeks, followed by a 3 month course of nebulised colistin, gentamicin or tobramycin). (D)
Discuss with patients the potential risks and benefits of starting eradication antibiotic treatment versus clinical observation following a new growth of P. aeruginosa in the context of stable bronchiectasis. This will include consideration of the likelihood of achieving sustained eradication, the risk of developing chronic infection, and the risk of adverse events with each management approach. (D)
Offer patients with bronchiectasis associated with clinical deterioration and a new growth of methicillin-resistant S. aureus (MRSA) (1st isolation or regrowth in the context of intermittently positive cultures) eradication. This should be attempted especially in view of infection control issues. (D)
Good practice point
Send sputum for culture and sensitivity immediately before and at each clinical attendance following antibiotics prescribed for bacterial eradication to determine the outcome of treatment.
Research recommendation
A randomised control trial of P. aeruginosa eradication therapy is needed to determine the microbiological and clinical outcomes of eradication therapy.
Does antibiotic therapy improve outcomes in patients with an exacerbation of bronchiectasis?
Good practice points
A patient self management plan should be considered, an example is provided here https://www.brit-thoracic.org.uk/standards-of-care/quality-standards/bts-bronchiectasis-quality-standards/)
There should be prompt treatment of exacerbations and suitable patients should have antibiotics to keep at home.
Previous sputum bacteriology results can be useful in deciding which antibiotic to use. Table 6 highlights the first-line and alternative treatments for the common bacterial pathogens implicated in exacerbations of bronchiectasis.
Where possible, sputum (spontaneous or induced) should be obtained for culture and sensitivity testing prior to commencing antibiotics.
Empirical antibiotics can then be started while awaiting sputum microbiology.
Once a pathogen is isolated, antibiotics can be modified if there is no clinical improvement, with treatment guided by antibiotic sensitivity results.
In general, antibiotic courses for 14 days are standard and should always be used in patients infected with P. aeruginosa. Shorter courses may suffice in patients with mild bronchiectasis.
Intravenous antibiotics should be considered when patients are particularly unwell, have resistant organisms or have failed to respond to oral therapy (this is most likely to apply to patients with P. aeruginosa).
Common organisms associated with acute exacerbation of bronchiectasis and suggested antimicrobial agents- adults
What treatments improve outcomes in patients with bronchiectasis and allergic broncho-pulmonary aspergillosis?
Recommendations
Offer oral corticosteroid to patients with active ABPA. An initial dose of 0.5 mg/kg/d, for 2 weeks is recommended. Wean steroids according to clinical response and serum IgE levels. (D)
Consider itraconazole as a steroid sparing agent for patients dependent on oral corticosteroids where difficulty in weaning is experienced. (B)
Monitor patients with active ABPA with total IgE level to assess treatment response. (C)
Does immunoglobulin replacement treatment therapy improve outcomes in patients with bronchiectasis due to antibody deficiency?
Recommendations
Offer IgG therapy to all patients with common variable immune deficiency (CVID) and x linked agammaglobulnemia (XLA). (B)
Consider IgG therapy for patients with specific polysaccharide antibody deficiency and/or IgA deficiency or IgG subclass deficiencies with absent/impaired pneumococcal vaccine antibody responses who continue to have objective evidence of bacterial sino-pulmonary infection and progressive disease despite appropriate management of bronchiectasis. (C)
Good practice points
All patients receiving IgG replacement therapy should be under the joint care of a clinical immunologist and respiratory specialist in bronchiectasis
Offer patients receiving replacement IgG the choice of hospital or home-based therapy.
Research recommendation
Randomised controlled trials are needed to assess which patients with bronchiectasis would benefit from long term Immunoglobulin G replacement therapy alone or as an adjunct to long term antibiotic therapy- assessing the optimal dose of IgG replacement and identification of ideal trough IgG level to prevent recurrent infections.
Gastro-oesophageal reflux disease (GORD) and bronchiectasis
Recommendation
Treat GORD symptoms in patients with bronchiectasis according to existing NICE guidance319. (D)
Good practice points
GORD should be considered in patients with hiatus hernia, persistent coliforms in sputum samples or recurrent exacerbations with no other cause identified.
Investigate patients who may have gastro-oesophageal reflux according to local policies.
Consider the addition of prokinetic agents if symptoms of GORD increase with an airway clearance technique in sitting position. Avoid eating in the hour immediately prior to physiotherapy.
What is the prevalence of rhinosinusitis in patients with stable bronchiectasis and what are the outcomes of treatment?
Recommendations
The evaluation of patients with bronchiectasis should include assessment of symptoms of chronic rhinosinusitis. (D)
Patients with bronchiectasis and symptoms of rhinosinusitis should be evaluated and treated according to existing evidence-based treatment pathways. (D)
Should treatment of bronchiectasis be altered in the presence of co-morbidities?
Recommendations
Consider a trial of inhaled and/or oral corticosteroids in patients with bronchiectasis and inflammatory bowel disease (IBD). (D)
Ensure optimal control of asthma and allergies in patients with both bronchiectasis and asthma (D).
Monitor patients with co-morbid COPD and bronchiectasis as they are at higher risk of death. (D)
Patients with bronchiectasis and autoimmune conditions should be carefully assessed for autoimmune related lung disease and often require long term follow up in a secondary care setting. (D)
Patients with bronchiectasis who require disease modifying antirheumatic drugs (DMARDs) or biologics for rheumatoid arthritis should be referred to a chest physician for further assessment before treatment is started. (D)
How should we monitor bronchiectasis?
Recommendation
All patients with bronchiectasis should undergo routine monitoring in order to identify disease progression, pathogen emergence and modify treatment where necessary. (D)
Good practice points
Tailor the frequency of routine monitoring to the patient’s disease severity (see table 7).
Assess patients annually, and more frequently in more severe disease.
Perform pulse oximetry to screen for patients who may need blood gas analysis to detect respiratory failure.
A baseline CXR may provide a useful comparator in the event of clinical deterioration.
Routine monitoring tests
Is there a role for microbiological sensitivity testing?
Good practice points
Antibiotic sensitivity testing can be used to determine if resistance develops to either acute or long-term antibiotic treatment.
Where possible, treatment should be guided by antibiotic sensitivity results but is often empirical based on previous sputum bacteriology.
Some patients with an infective exacerbation may respond to antibiotic treatment despite resistance to that drug in vitro. Antibiotics should only be changed if there is no clinical response.
For those on long term antibiotic treatment, there should be repeat sensitivity testing where there is a clinical concern regarding loss of efficacy with therapy.
Is there any evidence of cross-infection with pathogenic organisms (conventional bacteria and environmental mycobacteria)?
Recommendations
Individual or cohort segregation based on respiratory tract microbiology results is not routinely required for patients with bronchiectasis. (D)
Good practice points
Good cross infection prevention principles should be applied: seek advice on local policies.
The transmissibility of P. aeruginosa in cystic fibrosis appears more common. In the case of shared facilities with cystic fibrosis patients the cross infection guidelines for cystic fibrosis should prevail.
Research recommendation
Large scale robust data that confirm or refute the transmissibility of key pathogens such as P. aeruginosa and non-tuberculous mycobacteria are needed.
Specialist vs non-specialist setting
Good practice point
Specialist clinics should be considered in patients requiring hospital follow up.
What are the complications of bronchiectasis?
Good practice point
If haemoptysis 10 mls or less over a 24 hour period, treat with an appropriate oral antibiotic. If clinical deterioration, arrange emergency admission to hospital.
Management of major haemoptysis should be multidisciplinary with involvement of respiratory physicians, interventional radiology and thoracic surgeons. Empirically treat patients with intravenous antibiotic therapy, based on their known microbiology, and consider adjunct treatment with tranexamic acid. Bronchial artery embolisation is the recommended first line treatment if significant haemoptysis persists.
Section 1
Introduction
The BTS Guideline for non-CF Bronchiectasis was published in 2010. At the time of publication it was agreed by the Guideline Group and the BTS Standards of Care Committee that work on an update to the guideline should begin soon after publication to ensure that the guideline recommendations remained current in the light of new evidence.
Since the Guideline was published, BTS has produced Quality Standards for bronchiectasis in adults, and has offered an annual national audit, and from 2012, both adult and paediatric audit tools have been available. The BTS Standards of Care Committee approved a proposal to revise and update the guideline in 2013.
For guidance on treatment for patients with non-tuberculous mycobacteria and bronchiectasis please refer to the BTS Guideline on the management of non-tuberculous mycobacterial pulmonary disease.1
The guideline covers adult bronchiectasis. CF bronchiectasis is excluded from the scope of the guideline. Paediatric bronchiectasis was also excluded due to the difference in aetiology and approach in this group.
Target audience for the guideline
This guideline is aimed at all healthcare practitioners who are involved in the care of patients with bronchiectasis: this will include primary care clinicians (GPs, practice and district nurses), and hospital specialist teams in infectious disease, respiratory medicine (respiratory nurse specialists, respiratory physiotherapists, pharmacists, physicians and surgeons), microbiologists, and radiologists.
Groups covered
Adults
Groups not covered
The following patient groups and areas are excluded:
Patients with CF-bronchiectasis
Children up to and including 15 years old
Scope of the guideline
The guideline covers:
Introduction section on prevalence;
Diagnosis of bronchiectasis;
Causes;
Investigations and management in particular for CF, ABPA, common variable immune deficiency, NTM, coexistent asthma, COPD, ILD.
A stepwise management plan which sets out investigation and treatment of bronchiectasis patients according to severity
Definitions of severity of disease
Areas not covered by the guideline
Cystic Fibrosis, Non-tuberculous mycobacterial pulmonary disease
Definition
This guideline refers to the investigation and management of patients with symptoms of persistent or recurrent bronchial sepsis related to irreversibly damaged and dilated bronchi, namely clinical bronchiectasis. It does not cover the management of cystic fibrosis (CF) and, for the purposes of the guideline, ‘bronchiectasis’ is synonymous with the term ‘non-CF bronchiectasis’. Likewise, it does not focus on traction bronchiectasis secondary to other lung pathologies, particularly the interstitial lung diseases, where bronchiectasis is commonly asymptomatic.
Section 2
Methodology
This guideline is based on the best available evidence. The methodology used to write the guideline adheres strictly to the criteria as set by the AGREE collaboration, which is available online www.agreetrust.org/resource-centre/agree-ii/. The British Thoracic Society Standards of Care Committee guideline production manual is available at http://www.brit-thoracic.org.uk/guidelines-and-quality-standards/.
Clinical questions and literature search
Clinical questions were structured in the PICO (Patient, Intervention, Control, Outcome) format, (online appendix 1) to define the scope of the guideline and inform the literature search.
Appendix 1
Systematic electronic database searches were conducted in order to identify potentially relevant studies for inclusion in the guideline. For each topic area the following databases were searched: Ovid MEDLINE (including MEDLINE In Process), Ovid EMBASE, and the Cochrane Library (including the Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects) from 1980.
The searches were first run in June 2014 and updated in June 2016 (see online appendix 2 for search strategy). Searches included a combination of indexed terms and free text terms and were limited to English language publications only. The initial search identified 3848 potential abstracts and the second search 1021 abstracts.
Appraisal of literature
Appraisal was performed to be compliant with the AGREE collaboration. Three individuals (AH, AS, ML) read the title and abstract of each article retrieved by the literature searches and decided whether the paper was definitely relevant, possibly relevant or not relevant to the project. Criteria formulated for categorising the abstracts into these three groups were:
Whether the study addressed the clinical question.
Whether the appropriate study type was used to produce the best evidence to answer the clinical question.
Review articles were excluded.
Abstract was in English.
Abstracts were not rejected on the basis of the journal of publication, country in which the research was performed or published nor the date of publication.
The screened abstracts were allocated to the relevant section(s) of the guideline and two group members allocated to each guideline section. The full paper was obtained for all relevant or possibly relevant abstracts.
The first screening process identified 1022 of the initial 3848 reference abstracts to be definitely or possibly relevant to the guideline. Two guideline reviewers per section independently reviewed the abstracts to identify papers to be appraised for the guideline. The two reviewers for each section then independently appraised each paper assigned to them using the Scottish Intercollegiate Guidelines Network (SIGN) critical appraisal checklists. The reliability of the evidence in each individual study was graded using the SIGN critical appraisal check lists and is shown in the evidence tables (++,+or -). The body of evidence for each recommendation was summarised into evidence statements and graded using the SIGN grading system (see table 2).
Levels of evidence
Disagreements were resolved by discussion with the section partner. The second literature search in June 2016 yielded 1021 abstracts. Of these, 277 were identified as definitely or possibly relevant to the guideline. However, of the 277 identified, all relevant abstracts from this search had been identified by the Guideline Development Group (GDG) in the intervening time and incorporated.
Considered judgement and grading of evidence
The Guideline Development Group used the evidence tables to judge the body of evidence and grade recommendations for this guideline. Evidence tables (web appendix 3) are available online. Where evidence was lacking to answer the formulated clinical questions, expert opinions were obtained through consensus. The following were considered in grading of the recommendations:
The available volume of the body of evidence.
How applicable the obtained evidence was in making recommendations for the defined target audience of this guideline.
Whether the evidence was generalisable to the target population for the guideline.
Whether there was a clear consistency in the evidence obtained to support recommendations.
What the implications of recommendations would be on clinical practice in terms of resources and skilled expertise.
Cost-effectiveness was not reviewed in detail as in-depth economic analysis of recommendations falls beyond the scope of this guideline.
Recommendations were graded from A to D as indicated by the strength of the evidence as shown in table 3. In line with SIGN guidance, ‘minus’ evidence was considered in context but in the absence of other ‘plus’ supporting evidence, it was discussed among the GDG regarding that point and any recommendation hence made was Grade D. Important practical points lacking any research evidence, nor likely to be research evidence in the future were highlighted as ‘Good Practice Points’ (GPP).
Grades of recommendation
Research recommendations are also provided and the overall research questions are presented in PICO format in appendix 8.
Appendix 8
Drafting the guideline
The Guideline Development Group corresponded regularly by email and meetings of the co-chairs sub group and full group were held in January, May and June 2014, January, May, September and December 2015, January, April, December 2016, January and November 2017. A number of teleconferences were also held. The BTS Standards of Care Committee (SOCC) reviewed the draft guideline in November 2017. The draft guideline was made available on-line March – April 2018 for public consultation and circulated to all the relevant stakeholders. The BTS SOCC re-reviewed the revised draft guideline in June 2018 and final SOCC approval granted in July 2018.
This BTS Guideline will be reviewed within 5 years from the publication date.
Guideline group members and declarations of interest
All members of the Guideline Group made declarations of interest in line with the BTS Policy and further details can be obtained on request from BTS. Guideline Development Group members are listed in appendix 1.
Stakeholders
The following organisations contributed to the consultation exercise:
ACPRC, ARNS, ARTP, BGS, BSTI, Edge Hill University, PCRS-UK, ProAxsis Ltd, RCN, RCP Edinburgh, Trudell Medical.
Section 3
How common is bronchiectasis?
UK data in 2013 revealed the prevalence in women was 566/100 000 and in men 486/100 0004.
Data from 12 US states over the period 1993–2006 demonstrate an average annual age-adjusted hospitalisation rate of 16.5 hospitalisations per 1 00 000 population. Women and those aged over 60 years had the highest rate of hospitalisations.2 New Zealand hospital admission rates are reported as 25.7 per 100 0003 highest in childhood and the elderly, and related to sex, socioeconomic deprivation and race.
Regarding co-morbidity coding that may provide information on aetiology, the UK data found no significant co-morbidity in 34% of patients, and the most common coded co-morbidities to be asthma (42%) and COPD (36%).4 HIV was coded in 7%, rheumatoid arthritis in 6%, other connective tissue disease in 5%, inflammatory bowel disease in 3% and antibody deficiency in 1%.
Section 4
How should the diagnosis of bronchiectasis be determined?
Imaging
There are no randomised controlled trials comparing different imaging techniques in establishing a diagnosis of bronchiectasis but there are several cohort studies of low to moderate quality as well as case series. Compared with HRCT sensitivity of CXR was 87.8% and specificity 74.4%.5 Compared with bronchography, thin section CT performed with 10 mm interspaces demonstrated a high accuracy in diagnosing bronchiectasis with false positive and negative rates for CT were 1% and 2% respectively.6 Volumetric CT has improved sensitivity and interobserver agreement compared with incremental/interspaced thin slice CT.7 8 Bronchiectasis was identified more commonly in helical than incremental thin slice images. Interobserver agreement was significantly better on a per segment basis with helical CT (kappa 0.87) than incremental (kappa 0.71), but radiation dose of helical CT was 3.4 times higher. Multidetector CT (MDCT) yielded higher sensitivity and specificity for the detection of bronchiectasis. Using MDCT as the reference standard and analysing data on a per lobe basis the sensitivity, specificity, positive and negative predictive values for incremental HRCT were 71%, 93%, 88% and 81% respectively. Interobserver agreement was also higher for MDCT.9
While the dose using volumetric CT using the same parameters is increased in comparison to incremental/interspaced images modifications of technique enable improved diagnostic accuracy with similar radiation dose.7–9 Jung et al concluded that low dose CT at 40mAs provides more diagnostic information in the evaluation of bronchiectasis than incremental HRCT.10
While clearance of inhaled radiolabeled tracers from the lung is impaired in bronchiectasis this is non-specific and seen in other airways disease so cannot be considered diagnostic of bronchiectasis. Chronic bronchitis, bronchiectasis and asthma were all associated with slower clearance of inhaled radiolabeled tracers than healthy non-smokers (P<0.005) with overlap between these disease groups.11
Currie et al assessed radio-aerosol tracheobronchial clearance in first 6 hours in bronchiectasis (12 patients), COPD with sputum (7), COPD without sputum (8) and healthy controls.10 In bronchiectasis tracheobronchial clearance of inhaled radiolabeled tracers was significantly lower than controls but similar to COPD patients.
Ashford et al showed that ventilation scintigraphy with 99mTc DTPA in 20 patients with suspected bronchiectasis had low sensitivity for bronchiectasis (56%) using bronchography as the reference standard.13
Evidence statements
Chest radiography (CXR) has limited sensitivity and specificity in diagnosing bronchiectasis particularly in mild disease (2+).
Compared with bronchography thin section CT performed with 10 mm interspaces has a high accuracy in diagnosing bronchiectasis. (2+)
Volumetric CT has improved sensitivity and interobserver agreement compared with incremental/interspaced thin slice CT. (2+)
Using modifications of technique radiation dose of volumetric CT can be reduced to comparable levels to incremental imaging while providing higher accuracy. (2+)
While clearance of inhaled radiolabeled tracers from the lung is impaired in bronchiectasis this is non-specific and seen in other airways disease so cannot be considered diagnostic of bronchiectasis. (2-)
Recommendations - Imaging
Perform baseline chest X-ray in patients with suspected bronchiectasis. (D)
Perform a thin section CT to confirm a diagnosis of bronchiectasis when clinically suspected. (C)
Perform baseline imaging during clinically stable disease as this is optimal for diagnostic and serial comparison purposes. (D)
Good practice points
CT imaging protocol
The most appropriate imaging protocol will vary according to scanner technology and patient factors.
When using volumetric CT, dose reduction techniques including adaptive mA and kV and iterative reconstruction should be utilised where available.
Typical CT imaging parameters for the diagnosis of bronchiectasis are:
Slice thickness:≤1 mm
Reconstruction algorithm: – high spatial frequency
kVp: 100–140
mAs (or effective mAs): 100–200
Gantry rotation time:<0.5 s
CT features of bronchiectasis
Bronchiectasis is defined by bronchial dilatation as suggested by one or more of the following:
Bronchoarterial ratio >1(internal airway lumen vs adjacent pulmonary artery)
Lack of tapering
Airway visibility within 1 cm of costal pleural surface or touching mediastinal pleura.
The following indirect signs are commonly associated with bronchiectasis:
Bronchial wall thickening
Mucus impaction
Mosaic perfusion/air trapping on expiratory CT
General
CT scanning can also aid in identifying an aetiology of bronchiectasis for example, ABPA, NTM, primary ciliary dyskinesia, alpha one antitrypsin deficiency, Williams Campbell syndrome and a foreign body.
Section 5
In whom should the diagnosis of bronchiectasis be suspected?
The most common symptom in bronchiectasis is cough particularly with sputum production.14 15
Appendices 5 and 6 show the causes identified from international studies. Often no cause is found despite aetiological testing. Past infection (such as measles, whooping cough, pneumonia or tuberculosis) and is a possible cause of bronchiectasis, particularly if persistent symptoms develop soon after the infection.
Appendix 5
Appendix 6
Specific disease groups with associated bronchiectasis
COPD
A meta-analysis of 6 observational studies found that the prevalence of bronchiectasis was 54.3% (range 25.6%–69%), more common in males (OR 1.62, 95% CI 1.15 to 2.28) and with a greater smoking history (weighted mean difference 4.63 pack years, 95% CI 1.61 to 7.65 pack years). Other features that distinguished patients with COPD and bronchiectasis from COPD alone included greater daily sputum production, higher exacerbation frequency, worse lung function, higher levels of inflammatory biomarkers, increased colonisation by potential pathogenic micro-organism (PPM) and increased rate of Pseudomonas aeruginosa (P. aeruginosa) colonisation.16 A systematic review and meta-analysis of 14 observational studies in COPD patients found that the presence of bronchiectasis was associated with worse airflow obstruction, isolation of PPM, increased risk of exacerbation and of mortality.17
Alpha-1 antitrypsin deficiency (A1AT)
A retrospective cohort study between 1995 and 2002 of 74 patients with PiZZ deficiency (mean age 50.6, SD 9.2 years) found radiological evidence of bronchiectasis in 94.5%.18 Another retrospective cohort study of 26 Irish patients with A1AT deficiency found that 14 had bronchiectasis, all of whom had PiZZ phenotype.19
Asthma
A careful cross-sectional analysis of 85 patients in secondary care with bronchiectasis found asthma in 27% of the clinic population while prevalence of asthma in the general population was 7%.20 A large study of patients with difficult asthma found bronchiectasis on CT scan in 40% of selected patients; the criteria for scanning were not stated but the scanned patients were older, with a longer duration of disease, on more corticosteroid treatment and with poorer lung function and more neutrophilic airway inflammation on sputum cytology than those who were not scanned.21 In a case-control study matching patients with steroid-dependent asthma to those managed without regular oral corticosteroids, it was noted that bronchiectasis was much more common in the former group and the overall prevalence of otherwise unexplained bronchiectasis was 12% across both groups, rising to 20% in the steroid-dependent group.22
Rhinosinusitis
Rhinosinusitis is common in bronchiectasis patients,23 but only one study appears to have assessed the prevalence of bronchiectasis in chronic sinusitis, finding it in 3 out of 60 patients (5%).24
Chronic systemic infection
Chronic infection such as HIV or HTLV-1 appears to increase the risk of bronchiectasis.25 26 27 28
Rheumatoid arthritis
Clinical studies of patients with rheumatoid arthritis (RA) have found varying rates of bronchiectasis on CT scan ranging from 4% to 58%.29–38
The diagnosis of bronchiectasis may occur in early or established RA, and presentation and diagnosis with bronchiectasis may pre-date the diagnosis of even seropositive RA. Significantly more erosive changes were observed on hand and foot radiology in 53 patients with bronchiectasis and RA versus 50 patients with RA alone, and both rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies were higher in those with bronchiectasis.39 In that study, bronchiectasis preceded the onset of RA in 58%.39
A large study on patients hospitalised with RA established the frequency of appropriate symptoms first and then investigated with CT scan. Out of 453 patients questioned, 13 had symptoms suspicious for bronchiectasis and 9 of the 10 patients scanned had confirmed bronchiectasis, giving a prevalence of 2.9% of symptomatic bronchiectasis in this population.40
Other connective tissue diseases
Bronchiectasis has been noted in other connective tissue diseases including primary Sjogren’s syndrome, Marfan’s syndrome, systemic sclerosis, systemic lupus erythematosus, and ankylosing spondylitis.
A study of a 507 patient cohort with primary Sjogren’s syndrome (PSS) identified 120 patients with suspected pulmonary disease, and found bronchiectasis on CT scan in 50 patients.41 Retrospective studies confirm the association.42–44
A retrospective review of 79 patients with Marfan’s who underwent HRCT imaging found evidence of bronchiectasis in 28%.45 Airway dilatation was described as not severe, often confined to one lobe and was said to localise with anatomical abnormalities such as pectus excavatum, although fibrosis due to previous tuberculosis was noted in some patients.45 Studies in ankylosing spondylitis have found incidence of bronchiectasis to range from 7.2% to 51.2%.46–51 In 7 of 34 patients with systemic lupus erythematosus (SLE) who prospectively underwent HRCT imaging, bronchiectasis was observed.52 A small study of systemic sclerosis found a high rate of bronchiectasis on CT in 13 (59.1%) of 22 patients.53 In a study of scleroderma and pulmonary hypertension, bronchiectasis independent of interstitial lung disease (ILD) was found on CT scan in 6 of 44 patients with restrictive lung function or crackles.54
Inflammatory Bowel Disease
There is a recognised association between bronchiectasis and inflammatory bowel disease (IBD). A prospective study of 95 patients with IBD (83 ulcerative colitis (UC) and 12 Crohn’s disease (CD)) who underwent HRCT scans found evidence of bronchiectasis in 9, all of whom had UC and no reported respiratory symptoms.55 A cohort study of 30 UC and 9 CD patients undergoing CT scans found bronchiectasis in two patients.56 In 36 consecutive IBD patients (23 UC, 13 CD) studied for pulmonary disease, bronchiectasis was found on CT in three patients. 44% of the total study population had respiratory symptoms, but sputum production was described in only two patients- the relationship between symptoms and CT findings was not described.57 A literature review found bronchiectasis in 44 out of 155 patients with inflammatory bowel disease.58
A retrospective case note review of 10 patients with IBD (5 UC, 5 CD) and bronchiectasis found that eight had developed respiratory symptoms only following surgery for their IBD.59 These patients had had IBD for a median of 15 (9-35) years and for those developing pulmonary symptoms following surgery, the time from surgery to symptoms ranged from 2 weeks to 30 years.59 In a study of 17 IBD patients with respiratory symptoms, the diagnosis of IBD preceded the onset of their pulmonary symptoms in 16. 13 of these patients were found to have bronchiectasis.60
Evidence statement
Studies in healthy populations do not provide a strong body of evidence but suggest that persistent mucopurulent or purulent sputum production in the stable state is suspicious for underlying bronchiectasis, particularly if there is a past history of major respiratory infection (eg, measles, whooping cough, pneumonia, tuberculosis) or ongoing rhinosinusitis (2-).
There is a high frequency of bronchiectasis in patients with COPD (2++), particularly with more severe airflow obstruction (2++).
The presence of bronchiectasis in patients with COPD is typically associated with chronic productive cough, isolation of PPMs from sputum, particularly P. aeruginosa, increased airway inflammation, frequent or severe exacerbations or admissions to hospital for exacerbations (2+).
Bronchiectasis is associated with alpha one antitrypsin deficiency, particularly with the phenotype PiZZ (2+)
Asthma is found in higher prevalence in patients with bronchiectasis than in the general population, (2+), and bronchiectasis appears more common in asthma, particularly in difficult to treat disease (2-).
There is an association between rheumatoid arthritis and bronchiectasis (2+). The diagnosis of bronchiectasis may precede the onset of rheumatoid arthritis (2-).
There is an association between bronchiectasis and other connective tissue diseases (2-).
There is an association between inflammatory bowel disease and bronchiectasis (2+).
Bronchiectasis has been reported in patients with HIV infection at a frequency higher than in the general population (2-).
Bronchiectasis has been reported in patients with HTLV-1 infection with inflammatory complications at a frequency higher than in the general population. (3)
Recommendations
Consider investigation for bronchiectasis in patients with persistent production of mucopurulent or purulent sputum particularly with relevant associated risk factors. (D)
Consider investigation for bronchiectasis in patients with rheumatoid arthritis if they have symptoms of chronic productive cough or recurrent chest infections. (C)
Consider investigation for bronchiectasis in patients with COPD with frequent exacerbations (two or more annually) and a previous positive sputum culture for P. aeruginosa while stable. (B)
Consider investigation for bronchiectasis in patients with inflammatory bowel disease and chronic productive cough. (C)
Good practice points
In at risk groups, if bronchiectasis is suspected, bronchiectasis needs confirmation.
In patients with COPD, investigation for bronchiectasis may be appropriate especially in the presence of chronic productive cough with positive sputum cultures for PPM while stable or two or more exacerbations in the preceding 12 months.
In patients with asthma, investigation for bronchiectasis may be appropriate with severe or poorly-controlled disease.
In patients with a history of HIV-1 infection, solid organ and bone marrow transplant, and history of immunosuppressive therapy for lymphoma and vasculitis, investigation for bronchiectasis may be appropriate with symptoms of chronic productive cough or recurrent chest infections.
In patients with chronic rhinosinusitis, investigation for bronchiectasis may be appropriate with symptoms of chronic productive cough or recurrent chest infections.
In patients with other connective tissue disease or inflammatory bowel disease, investigation for bronchiectasis may be appropriate if they have symptoms such as chronic productive cough or recurrent chest infections.
Investigation for bronchiectasis may be appropriate in otherwise healthy individuals with a cough that persists for longer than 8 weeks, especially with sputum production or a history of an appropriate trigger (see BTS Recommendations for the management of cough in adults61).
Section 6
Investigations for causes of bronchiectasis
Introduction
Single centre studies have shown that investigations into the underlying cause of bronchiectasis can change patient management in a significant proportion of cases (5%–37%) and identify previously unrecognised conditions such as allergic bronchopulmonary aspergillosis (ABPA), primary antibody deficiency syndromes and cystic fibrosis (CF) which have important therapeutic and prognostic implications.23 62–66 Early studies were conducted in specialist centres but more recently studies of adult patients have been conducted in general chest clinics; online appendix 5 summarises those most relevant to the UK population and includes a systematic review of 56 studies covering 8608 patients from across the world.67
Review of imaging can suggest possible aetiologies although the reliability of this approach has not been formally assessed. For example disease in a single lobe might be due to obstruction from tumour or foreign body, and bronchoscopy would be an appropriate investigation in such cases. Post-tubercular disease might be supported by distribution or the presence of calcification. A diagnosis of post-infective disease would be supported by onset of symptoms soon after the illness. Bronchiectasis following measles or whooping cough is often bilateral and lower lobe.
It can be difficult to ascertain if conditions such as COPD, rheumatoid arthritis, inflammatory bowel disease or GORD are causative of bronchiectasis. Even with an obvious apparent aetiology, there may be value in carrying out standard investigations at baseline, since patients with established disease may later develop an immunodeficiency or ABPA.
Standard laboratory tests
The evidence for the role of aetiological investigations is derived from studies of low to moderate quality; other significant limitations include a lack of standardised diagnostic testing panels for bronchiectasis, resulting in marked variation in the performance of some diagnostic assays (CF mutation analysis, test immunisation of vaccine responses), use of different technological platforms for some diagnostic assays which may give rise to discrepancy in test results (measurement of pneumococcal and aspergillus IgG antibodies) and variation in the use of reference intervals to define presence or absence of disease even when using same or very similar diagnostic tests (Aspergillus blood IgE levels).
Although most individual studies are of low/moderate quality, the overall findings indicate that antibody deficiency syndromes and ABPA should be investigated in all newly presenting patients with bronchiectasis (see appendix 5).
Tests for specific disease groups with associated bronchiectasis
Allergic bronchopulmonary aspergillosis
Data suggests that this is a common cause of bronchiectasis in the UK, between 1% and 11% in UK series.23 62 63 68 69
The diagnostic criteria for ABPA are well established for asthma and have been modified for cystic fibrosis.70 They include a history of asthma, evidence of Aspergillus fumigatus (A. fumigatus) IgE sensitisation on blood and/or skin tests, elevated total IgE levels and eosinophil counts, detection of Aspergillus precipitins or IgG, isolation of A. fumigatus in sputum cultures, presence of pulmonary infiltrates on chest x rays and distribution of bronchiectasis on CT chest scans.71–73 The presence of high attenuation mucus on CT scan may be useful in diagnosis and in staging the severity of ABPA.74 ABPA is an aetiology for bronchiectasis, and may be a complicating factor in established disease. Inconsistent diagnostic criteria have been used in the previously cited studies of aetiology of bronchiectasis.23 62–65 75 76 There are no studies in patients presenting with bronchiectasis that can help to establish the optimal number of investigations and the most important criteria for a diagnosis of ABPA in this context; criteria for asthma are generally used.
Sensitisation to A. fumigatus can be detected using blood specific IgE or skin tests however there is limited evidence on which method is best. Intradermal skin tests are more sensitive than standard skin prick to detect Aspergillus-specific IgE,77 but interpretation can be difficult and they are most used in academic centres with a specialist interest. A recent single centre specialist care study from India which used latent class analysis (the statistical test used to assess diagnostic test performance in conditions without a diagnostic gold standard) showed that detection of Aspergillus-specificIgE in blood was more sensitive than intradermal skin tests for the diagnosis of ABPA.78
Diagnostic criteria for ABPA include positive IgE blood and cutaneous skin test results as there may be a small proportion of patients who have discrepant blood and skin test results.73 Use of blood rather than cutaneous skin test has the advantage that patients on anti-histamines do not need to stop treatment, and quality data on laboratory performance is more widely available than on skin testing. IgE sensitisation to A. fumigatus has been reported in 19% of unselected patients presenting with bronchiectasis using blood tests62 however the optimal concentration required to diagnose ABPA in bronchiectasis cohorts has not been established.23 62 64
Similarly the use and definition of raised total IgE blood tests in diagnosis of ABPA has been variable in bronchiectasis cohorts.23 62–64 The earliest available total IgE test should be used, as the total IgE concentration declines significantly with remission of ABPA on oral corticosteroids whereas no consistent effects on Aspergillus-specific IgE occur.79 There is no consensus on what value of IgE is required for diagnosis of ABPA. In a single specialist centre study the sensitivity of an IgE concentration more than 1000IU/ml for diagnosis of ABPA in asthmatic patients was 97.5%.78 A normal IgE level in a corticosteroid naïve patient with bronchiectasis means that ABPA is highly unlikely. A combination of testing for Aspergillus-specific IgE and total IgE has been proposed as the most sensitive way to screen for ABPA in patients with asthma, with secondary more specific tests to confirm the diagnosis78; this approach has not been validated in patients with bronchiectasis.
An eosinophil count above 1.0×109/L is a major criterion for ABPA78 but should be used as a second line test as normal counts do not exclude this disease80 and there is no significant difference in eosinophil counts between patients with A.fumigatus sensitisation and those with ABPA.81 Previous studies in asthmatic patients have all been conducted in a single centre and have relied on manual eosinophil counts which are less accurate than automated diagnostic platforms.78–81
Aspergillus-specific IgG antibodies can be found in 70%–90% of patients with ABPA using agar gel immune diffusion technology.82 83 The results of these studies may not be applicable to current epidemiology of A. fumigatus ABPA, as a recent study showed that the diagnostic performance of the Ouchterlony diffusion technique to detect IgG antibodies had declined and Aspergillus precipitins were only seen in 43% of patients with ABPA.78 In addition immunoprecipitation techniques to detect Aspergillus-specific IgG antibodies are not widely available in diagnostic UK laboratories, having been replaced initially by counter immuno-electrophoresis (CIE) initially and more recently by ELISA. Only one study of aetiology in bronchiectasis63 defined criteria for a positive Aspergillus precipitins test result and diagnostic techniques used to determine presence of Aspergillus-specific IgG antibodies were not described by any investigators. A small UK study comparing the diagnostic test of CIE and ELISA in patients with Aspergillus related lung disorders showed that the sensitivity of ELISA (41%–46%) for ABPA was significantly greater than CIE (15%) however lack of relevant disease control group and absence of data of current anti-fungal therapy make it difficult to ascertain the clinical value of Aspergillus-specific IgG detection using current diagnostic techniques.84 Aspergillus precipitins can be raised in other conditions such as aspergilloma and chronic pulmonary aspergillosis and thus the more likely diagnostic role if any for Aspergillus-specific IgG antibodies will be as a second line confirmatory test.
Culture of A. fumigatus from lung secretions is supportive but not diagnostic of ABPA as this fungus can be isolated in a number of other diseases. Rate of positive sputum cultures in historical cases of ABPA ranges from 63%–97%,82 83 however in the only study of aetiology of bronchiectasis in which sputum cultures were part of the standard diagnostic panel, A. fumigatus was only isolated in 9% of cases of ABPA.62 Reasons for lower yields of A. fumigatus in sputum cultures could include exposure to azole therapy and differences in sputum processing and culturing technologies in microbiology laboratory services.85
In the absence of stronger evidence, all the following criteria based on expert consensus are suggested for steroid naïve patients.
Associated clinical deterioration (increased cough, wheeze, increased sputum production, worsening lung function, exacerbations)
Total serum IgE level >500 IU/mL (or ku/L)- precise cut-off is not known.
Immediate cutaneous reaction to Aspergillus (skin prick test weal of >3 mm in diameter with surrounding erythema, patient not on systemic antihistamines at the time).
Increased Aspergillus species specific IgE antibodies
New radiological infiltrates and/or high attenuation mucus plugging. In later stages, proximal bronchiectasis develops.
Supportive findings include peripheral blood eosinophilia, and Aspergillus precipitins.
Immune dysfunction
Immune deficiency occurred in 5.8% of patients in a multi-centre cross sectional European study63 and in 5% of patients in a large systematic review of aetiological studies.67 In adults, almost all cases of immune deficiency are likely to involve defects in antibody production. Recognition of significant antibody syndromes such as common variable immune deficiency (CVID) is important as immunoglobulin replacement therapy can reduce exacerbation frequency and improve clinical outcomes.86 In recent years there has been increasing recognition that treatment for haematological malignancies is associated with increased risk of antibody deficiency syndromes and bronchiectasis65 which may respond well to immunoglobulin replacement.87
Serum immunoglobulins (IgG, IgA, & IgM) and electrophoresis
A polyclonal rise in serum IgG and IgA is commonly seen in patients with bronchiectasis and reflects chronic infection and inflammation.64 There are no studies addressing the clinical utility of serum electrophoresis in the investigation of bronchiectasis, but this test is essential to determine whether raised serum immunoglobulins are polyclonal or monoclonal. The presence of a monoclonal immunoglobulin in serum needs further investigation to diagnose myeloma, Waldenstrom’s macroglobulinaema, chronic lymphatic leukaemia and monoclonal gammopathy of uncertain significance (MGUS). The prevalence of MGUS is 3.2% in individuals over the age of 50 with increased rates in males, older age and African Americans.88 B cell lymphoproliferative disorder and MGUS are associated with increased rates of bacterial chest infections89 and patients need appropriate follow-up to monitor for haematological malignancy. Antibody deficiency secondary to B cell lymphoproliferative disorders has been found in a number of studies examining aetiology of bronchiectasis,23 65 although the presence or absence of immunoglobulin monoclonal proteins was not stated.
Isolated reduction in IgG, IgA and IgM is not uncommon62 64 76 90 and will usually require further evaluation to assess clinical significance in management of bronchiectasis. Minor reduction in IgG and IgM can be secondary to steroid therapy, B cell lymphoproliferative disease or unclassified antibody deficiency syndromes, which may require further specialised investigation (assessment of vaccine responses, lymphocyte immune phenotyping and enumeration of lymphocyte subsets) and/or involvement of other medical specialists to manage relevant co-morbidity.
Full blood count (FBC)
There are no studies examining the clinical utility of FBC in determining the cause of bronchiectasis but an abnormal profile may give important diagnostic clues. Persistent low neutrophil and lymphocyte counts in patients with stable disease may suggest an underlying secondary or primary immune deficiency. Lymphocytosis can be a marker of B cell lymphoproliferative disease and a raised eosinophil count may support a diagnosis of ABPA. Reduced platelet count can be a feature of primary and secondary immune deficiencies whereas thrombocytosis is associated with active RA and IBD.
Measurement of baseline specific antibody levels against capsular polysaccharides of Streptococcus pneumoniae
Measurement of functional antibody responses to T cell dependent protein or glycoprotein antigens and T cell independent polysaccharide antigens is an essential criterion for diagnosis of primary antibody deficiency syndromes including CVID and specific polysaccharide antibody deficiency (SAD).91 92 Assessment of functional antibody responses is also indicated to assess clinical significance of partial/total IgA deficiency, isolated reductions in IgG and IgM, reduced IgG and IgM and reduced immunoglobulin isotypes in patients with B cell lymphoproliferative disorders. In clinical practice, analysis of T cell independent antigen response is usually assessed by measurement of pneumococcal antibodies, which is also clinically relevant in patients with bronchiectasis.
The initial step to investigate functional antibody response is to measure pneumococcal antibody levels, and if low, to immunise with 23 valent carbohydrate Pneumococcal vaccine and check post vaccine level 4–8 weeks later. Antibody levels below protective threshold are deemed to be indicative of impaired vaccine responses and functional antibody deficiency.
The proportion of unselected bronchiectasis patients with reduced levels of pneumococcal antibodies varies between 2%–21%.23 62–64 Differences in reported studies may relate to study setting, differences in pneumococcal antibody assays, or the pneumococcal antibody level at which test immunisation was considered. Some studies reporting pneumococcal antibody levels in unselected patients with bronchiectasis63–66 do not distinguish between the need to assess the functional significance of reduced serum immunoglobulins in patients with bronchiectasis and the use of this test solely to screen for patients with SAD.
The optimal pneumococcal level at which test immunisation should be considered varies: criteria for test immunisation have included patients with baseline pneumococcal antibody levels in the lowest fifth centile23 or 25th centile62 for healthy controls. Studies using in-house assays to measure total IgG response to pneumococcal immunisation have reported the largest number of patients with low pneumococcal antibody and reduced pneumococcal vaccine responses.62 93 Pneumococcal in-house assays have largely been replaced by commercial assays which may not give equivalent results, resulting in the need to define pneumococcal antibody reference intervals and decision points at which pneumococcal test immunisation is offered. There is currently a move towards serotype based assays of individual pneumococcal serotypes, usually 12–14 in total92 94 95 ; only a limited number of laboratories offer this test in the UK. In addition there is only moderate agreement between quoted protective levels based on gold standard ELISA and newer multiplex bead array diagnostic platforms and disagreement concerning use of protective antibody levels (invasive disease as opposed to mucosal infection).
Use of protein conjugate pneumococcal vaccine in childhood may alter dynamics of polysaccharide pneumococcal vaccination in adults.91 Bronchiectasis clinics and immunology laboratories need to have data on distribution of either total and/or individual serotype pneumococcal IgG levels in age- matched healthy controls and local agreement on the decision point used in pneumococcal antibody tests as to when patients with bronchiectasis are offered 23 valent polysaccharide vaccine test immunisation.
Reduced pneumococcal vaccine responses are part of the diagnostic criteria for a number of primary antibody deficiencies95 and have important implications for the use of immunoglobulin replacement therapy in patients with bronchiectasis with primary and secondary antibody deficiencies. There are no uniform criteria as to what constitutes a protective threshold antibody for total IgG pneumococcal (23 valent carbohydrate Pneumococcal vaccine) levels, however a post vaccine pneumococcal serotype concentration greater than 1.3 ug/mL is believed to offer protection against strain specific invasive pneumococcal disease.96 Expert opinion suggests that failure to generate a protective titre (1.3microG/microL) to more than 70% serotypes post polysaccharide pneumococcal vaccination is indicative of moderate to severe functional antibody deficiency.92 These criteria have not been validated in clinical trials and it has been argued they may overestimate the number of patients with functional antibody deficiency.
The rate of impaired post pneumococcal test immunisation responses in patients with bronchiectasis has varied from 0%–20%,23 62–65 93 with the main sources of variation being the nature of the patient cohort, different methodology in assessing the response, and variations in the definition of low baseline levels and a normal response. Criteria used to define adequate pneumococcal vaccine responses have included results obtained from post vaccine serology from healthy controls,93 use of historical reference data62 or expert opinion,65 however a number of studies have not reported their criteria to select patients for test immunisation, the test methodology and the definition of normal pneumococcal vaccine response.23 64 66
Interpretation of pneumococcal test immunisation results needs to take into account history of recent infections, previous vaccinations, use of immunosuppressive and cytotoxic chemotherapy and the finding that impaired pneumococcal test immunisation responses can be seen in up to 10% of healthy individuals. The increasing use of pneumococcal serotype assays for which there is no data for clinical utility in patients with bronchiectasis and limited agreement on what constitutes an adequate immune response91 suggest that there needs to be appropriate liaison between bronchiectasis clinics and diagnostic immunology services as to which patients should be offered test immunisation, what technology is used to measure pneumococcal antibodies, and what criteria are used to define a normal vaccine response.
Interpretation can be challenging and thus it is advised the results are discussed with an immunologist, as there has not been universal agreement about the degree of vaccine response to define specific antibody deficiency. If there is no local access to an immunologist, suggest discussion with a specialist bronchiectasis service that has an immunologist as part of the multi-disciplinary team.
More specialised immunological investigations are described in the appendix; these would usually be carried out by immunologists or in close liaison with immunology services (see appendix 4).
Appendix 4
Rheumatoid arthritis
Rheumatoid arthritis is the aetiology for a small proportion of patients referred to secondary care with bronchiectasis (2%–5%23 62 64). Given the strong association between rheumatoid arthritis and bronchiectasis, auto-antibodies such as rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies have been considered as aetiological tests. Presence of circulating RF in patients was shown to be more prevalent in patients with bronchiectasis compared with healthy controls in a prospective multi-centre case-control observational study.97 However anti-CCP antibodies were strongly positive in only 12% (4 patients) of those who were RF-positive. Two of those four patients subsequently developed rheumatoid arthritis in a 12 month follow-up period.
Recurrent aspiration
Recurrent aspiration due to dysphagia or gastro-oesophageal reflux is recognised to cause bronchiectasis, with a reported prevalence (based on the presence of symptoms) of between 1% and 11.3% in adults23 62 64 65 76 and a higher rate in a paediatric cohort attending a specialist referral centre.75 However, gastro-oesophageal reflux is common (and therefore can be mistakenly attributed as a causal factor), and can be asymptomatic (and therefore not considered). Limited case series are suggestive of a role for surgical management of reflux disease.98 99 Dysphagia can be caused by neurological disorders, oesophageal dysmotility and anatomical disorders (trachea-oesophageal fistula, previous surgery, pharyngeal pouch, late effects of head and neck radiotherapy). The likelihood of aspiration may be increased by vocal cord dysfunction. A careful gastrointestinal history focussing on symptoms of reflux and dysphagia should therefore be undertaken.
A number of different investigative modalities are available and include videofluoroscopic swallow study, upper gastrointestinal endoscopy, ambulatory oesophageal manometry and pH studies and flexible endoscopic evaluation of swallow. The sensitivity and specificity of these tests when used to assess aspiration in bronchiectatic patients have not been investigated. The method of evaluation should therefore be tailored according to clinical features.
Cystic fibrosis
Cystic fibrosis (CF) bronchiectasis is managed as a distinct clinical entity. Routine newborn screening for CF has been standard in the UK since 2007, but the disease may still present in later life and should be considered as a possible aetiology. CF is mainly seen in Caucasian populations and is rare in Asian populations.100 101 Clinical features supportive of CF include an early onset, history of malabsorption, male infertility and childhood steatorrhoea. Radiologically, upper lobe bronchiectasis predominates and there is frequently a history of Staphylococcus aureus on sputum culture.
Standard investigative methods for CF include the sodium chloride sweat test and CFTR mutation analysis. There are established guidelines for the sweat test which should measure chloride concentration on two occasions. A negative test has <30 mmol/L chloride, a borderline test 30–60 mmol/L and a positive test >60 mmol/L.102 103
The CFTR gene is located on chromosome seven and to date >2000 CFTR mutations have been identified (www.genet.sickkids.on.ca). It has been demonstrated that the greater the number of mutations screened, the greater the number of patients with CF will be identified.104 Advice from the local clinical genetics department should be sought. Ancillary tests such as nasal potential difference and assessments of pancreatic exocrine function offer additional evidence only and are not diagnostic in themselves. Their use should be limited to within specialist CF centres.
The incidence of CF as a cause in adults presenting with bronchiectasis ranges from 0.6%–2.7% (see online appendix 6).
For recommendations for the diagnosis and management of CF refer to the NICE CF Guidelines.105
Ciliary dysfunction
Primary Ciliary Dyskinesia
Primary ciliary dyskinesia is usually an autosomal recessive disorder causing ultrastructural defects in the cilia affecting normal motility. It is characterised by upper and lower respiratory tract infections, chronic sinopulmonary infection, development of bronchiectasis and loss of lung function. Male infertility is common and situs inversus may be present. Kartagener’s syndrome describes the classic triad of situs inversus, bronchiectasis and chronic sinusitis due to a congenital reduction or absence of ciliary function.
PCD is typically diagnosed in the paediatric population. The incidence of PCD as a cause of bronchiectasis in adults ranges from 0.9%–10.3% (see online appendix 6). Investigative methods that have been used are either screening tests including measurement of nasal nitric oxide (nNO) and the saccharin taste test, or diagnostic tests assessing ciliary structure and function. The saccharin taste test is no longer recommended in the investigative process for PCD.106 nNO levels are abnormally low in PCD.107–109 A large prospective study found the positive predictive value (PPV) of nNO (using a cut-off value of <30 nL/min) for a diagnosis of PCD to be 0.76 (CI 0.6 to 0.88) and the negative predictive value (NPV) 0.99(CI0.97–1.00) with a sensitivity of 91% and specificity of 96%.110 In a separate study, the PPV of nNO was 87% and NPV 97% in discriminating between PCD and non PCD bronchiectasis.111
Nasal brushing is a simple, minimally invasive method to obtain ciliated epithelium. Analysis of ciliary beat frequency and pattern is usually undertaken using high speed video microscopy analysis (HSVMA). Normal ciliary beat frequency (11–20 Hz) and ciliary beat pattern is a qualitative assessment. The PPV of HSVMA for a diagnosis of PCD has been shown to be 0.61 (CI 0.5 to 0.7) and NPV 1.0 (CI 0.99 to 1.00) in a major UK centre’s referral population, with a sensitivity of 100% and a specificity of 93%.110 Transmission electron microscopy (TEM) to assess ciliary ultrastructure has been shown to have a PPV of 1.00 (CI0.94–1.00) and a NPV of 0.95 (CI 0.92 to 0.97) with a sensitivity of 79% and specificity of 100%.110 Both HSVMA and TEM are excellent diagnostic tools but require expertise and specialist review. Further information is given in the ERS guidelines for the diagnosis of PCD.106
(Diagnostic centres for PCD testing in the UK are located in London (http://www.rbht.nhs.uk/patients/condition/primary-ciliary-dyskinesia/) Leicester (http://www.leicestershospitals.nhs.uk/), and Southampton (http://www.uhs.nhs.uk/OurServices/Childhealth/Primary-ciliary-dyskinesia/PCD-diagnostic-service.aspx).
Young’s syndrome
The combination of primary azoospermia, chronic rhinosinusitis and bronchiectasis was first briefly described in 1970 as the Berry-Perkins-Young Syndrome.112 Further studies suggested that this consisted of a specific form of obstructive azoospermia while the airway features included poor mucociliary clearance. Crossover with cystic fibrosis was ruled out113 and in general no specific ciliary beat frequency or ciliary ultrastructural abnormalities were identified,114 although a more detailed study in 1992 did find some minor abnormalities of ciliary function.115 It was proposed that Young’s syndrome was caused by childhood mercury exposure (also responsible for Pink disease (acrodynia) which is a recognised aetiology of bronchiectasis for some UK patients) on the grounds that the specific type of obstructive azoospermia reported in Young’s syndrome is becoming less common and epidemiologically this fits with the withdrawal of mercury-containing products such as teething powders in the UK and Australia.116 The role of Young’s syndrome in the aetiology of bronchiectasis may perhaps become of historical interest only.
Alpha-1 antitrypsin deficiency
PiZZ A1AT deficiency has been found in <1% of patients presenting with bronchiectasis.62 Insufficient information is given in aetiological studies to guide which bronchiectasis patients to investigate for A1AT deficiency.
Congenital causes
Congenital abnormalities causing bronchiectasis and presenting in adults are rare. Such congenital abnormalities may include Williams Campbell syndrome (bronchomalacia), Mounier Kuhn syndrome (tracheobronchomegaly) and lung sequestration.
The diagnosis of both Williams Campbell and Mounier Kuhn syndromes are made based on characteristic features on CT scanning of the chest.117 118 The data describing the incidence of these syndromes presenting in adulthood is limited to case reports or series.
Investigations of lung microbiology
The main role of sputum culture is to help guide the use of antibiotics both for treatment of acute exacerbations and for chronic suppressive therapy. In addition the detection of some micro-organisms may also help in identifying an underlying aetiology. For example isolation of environmental mycobacteria should prompt further investigations for the presence of non-tuberculous mycobacteria (NTM) pulmonary disease; finding Staphylococcus aureus might indicate the presence of cystic fibrosis; isolation of A. fumigatus may prompt investigations for ABPA.
There has not been a systematic analysis of the role of bronchoscopy in the diagnosis and management of bronchiectasis. However, it should be considered in those patients who do not expectorate especially in the context of infective change seen on CT. It may be particularly helpful in the diagnosis of NTM pulmonary disease. See appendix 7 for studies of lower respiratory tract micro-organisms.
Appendix 7
Evidence statements
It is sometimes possible to define an aetiological cause for bronchiectasis which directly alters management through the use of a standard panel of investigations. (2++)
Allergic bronchopulmonary aspergillosis (ABPA) occurs in 4% (range 1%–8%) of patients with bronchiectasis. (2+)
A diagnosis of ABPA is supported by total IgE >500 IU/mL (ku/L) and either positive Aspergillus-specific IgE or immediate reaction on skin prick testing. (4)
Antibody deficiency syndromes are found in 7% (range 2%–17%) of patients with bronchiectasis. (2+)
Cystic fibrosis is diagnosed in 3%–4% of adult patients with bronchiectasis. (1+)
Primary ciliary dyskinesia is diagnosed in the majority of studies in ≤5% of adult patients with bronchiectasis. (1+)
There is little evidence to support routine testing for autoimmune disease or alpha one antitrypsin deficiency in the absence of suggestive clinical features. (2++)
Serum rheumatoid factor is frequently positive in patients with bronchiectasis (2+) but the clinical significance of this is uncertain.
Aspiration is often associated with bronchiectasis (2+) and may be causally related. (4)
Recommendations (see table 1)
A panel of investigations should be performed to establish the underlying cause of bronchiectasis. (B)
Co-morbidities and past medical history should be recorded in patients diagnosed with bronchiectasis to identify relevant and possibly causative disease such as rheumatoid arthritis, COPD, asthma, gastro-oesophageal reflux disease and inflammatory bowel disease. (C)
Measure full blood count, serum total IgE and assessment of sensitisation (specific IgE or skin prick test) to A. fumigatus in all patients with bronchiectasis. (D)
Serum IgG, IgA and IgM should be performed in all patients with bronchiectasis. (C)
Consider measuring baseline specific antibody levels against capsular polysaccharides of S. pneumoniae in all patients to investigate for specific antibody deficiency. If pneumococcal antibodies are low, immunise with 23 valent polysaccharide pneumococcal vaccine, followed by measurement of specific antibody levels 4–8 weeks later.(D).
Test for cystic fibrosis (according to NICE Guidelines for CF) in patients with supporting clinical features, for example, early onset, male infertility, malabsorption, pancreatitis. (B)
Test for PCD (according to ERS Guidelines for PCD Diagnosis) in patients with supporting clinical features, including a history of neonatal distress, symptoms from childhood, recurrent otitis media, rhinosinusitis, or infertility. (A)
Sputum cultures should be performed in all patients with bronchiectasis for routine and mycobacterial culture. (D)
Good practice points
A previous diagnosis of idiopathic bronchiectasis should prompt careful reinvestigation for a primary cause in the context of a deteriorating clinical course or a young patient (usually considered to be age 50 and under but not limited to this age group).
Referral to a specialist centre for investigation should be considered for young patients (usually considered to be age 50 and under but not limited to this age group) and those with apparent idiopathic bronchiectasis especially where there is evidence of progressive disease.
Consider testing for RF, anti CCP, ANA and ANCA in patients with coexisting clinical features of arthritis, connective tissue disease and/or systemic vasculitis.
Consider testing for A1AT deficiency in patients with coexisting basal panacinar emphysema.
Investigations for reflux and aspiration should be undertaken only in symptomatic patients, or where there are other suggestive clinical features.
Consider bronchoscopy for patients with localised disease to rule out an endobronchial lesion or foreign body as the cause of bronchiectasis.
A bronchial aspiration or bronchial wash targeting the areas of bronchiectasis from CT scan of the chest should be considered in patients who do not expectorate and can be particularly helpful in the diagnosis of NTM pulmonary disease.
Serum protein electrophoresis should be performed in all patients with bronchiectasis with raised immunoglobulins.
Consider HIV-1 serology in patient with bronchiectasis depending on prevalence of HIV-1 and clinical features suggestive of increased risk of retroviral infection.
Research recommendations
Consensus criteria for diagnosis of ABPA need to be validated in bronchiectasis cohorts.
Consensus criteria for definition of abnormal post pneumococcal test immunisation antibody responses need to be validated in bronchiectasis cohorts.
Section 7
Prognosis: what is the outlook for these patients?
A UK epidemiology study examined mortality and noted the age adjusted mortality rate for women with bronchiectasis to be 1438 per 1 00 000 against 636 for the general population (comparative mortality of 2.26) and, in men, the age adjusted mortality rate for bronchiectasis population was 1915 per 1 00 000 compared with 895 for the general population (comparative mortality of 2.14).4
A comprehensive assessment by Martinez-Garcia et al119 2014 in Spanish patients comparable to the UK population introduced the mortality prediction score (FACED), based on a study showing that of 154 deaths during follow-up, 42.9% were attributed to respiratory disease with 9.1% due to neoplasia and 9.1% to cardiovascular disease.119 Similarly the Bronchiectasis Severity Index (BSI) tool was based on studies of outcome in patients with bronchiectasis across several different centres, and the study reported a mortality rate of 62 (10.2%), directly relevant to bronchiectasis in 32 cases (listed as exacerbation of bronchiectasis, end-stage bronchiectasis, pneumonia, LRTI, chronic respiratory failure or pneumothorax).120 Otherwise, myocardial infarction was the cause of death in 12 cases, malignancy in eight cases, and other causes included heart failure, stroke, other sepsis, pulmonary embolism, trauma, alcoholic liver disease and post-operative complications.
Section 8
Severity scoring
The availability of the two clinical scoring systems, the Bronchiectasis Severity Index (BSI) (table 4)120 and FACED119 (see tables 4 and 5), has increased our ability to predict future mortality in patients with bronchiectasis. The BSI additionally provides information on morbidity, hospital admissions and exacerbations. As bronchiectasis is not a rapidly fatal condition, these latter outcomes are regarded as more important for clinical decision making. Reassuringly, being derived in different cohorts, the two scores include similar variables. The major limitation of the FACED score is the absence of exacerbations which are regarded by many clinicians as the most important modifiable marker of severity. Prior exacerbations are also the strongest predictor of future exacerbations which explains why a number of studies have found FACED to be poorly predictive of future morbidity.121–123 For this reason the BSI is the preferred scoring system. At the time of writing, modifications of the FACED score to include exacerbations are undergoing evaluation. There may be some relevant omissions from both scores, notably the presence of co-morbidities which are important in the prognosis of other chronic respiratory diseases.
Variables involved in calculating the severity score in the Bronchiectasis severity index
Variables involved in calculating severity in the FACED score
FACED includes FEV1, Age, P. aeruginosa colonisation, Extent of bronchiectasis (counting lobar involvement on CT) and Dyspnoea (using the modified MRC scale). All the variables are dichotomised and scored 0 vs 1 or 2. The 5 year mortality in mild, moderate and severe disease (defined as a score of 0–2, 3–4 and 5–7 points respectively) is 4%, 25% and 56% respectively. It has been shown to predict 5 year mortality, although the study used the score calculated at the time of initial diagnosis (and is not, therefore, designed for follow-up of existing patients, an important limitation) and it is not known whether a change in score reflects a change in prognosis.
The BSI combines age, body mass index, FEV1, previous hospitalisation, exacerbation frequency, colonisation status and radiological appearances. The score was designed to predict future exacerbations and hospitalisations, health-status, and death over 4 years. Patients with NTM were excluded. Data were provided which examine how the score performed in annual prediction of events, a more relevant clinical scenario than provided for FACED, and the team have developed a useful online calculator (available at www.bronchiectasisseverity.com). A score of 0–4 (mild) is associated with 0%–2.8% mortality and 0%–3.4% hospitalisation rate over 1 year, and 0%–5.3% mortality and 0%–9.2% hospitalisation rate over 4 years.
Outcomes in moderate bronchiectasis (score 5–8) were 0.8%–4.8% mortality and 1.0%–7.2% hospitalisation rate at 1 year and 4%–11.3% mortality and 9.9%–19.4% hospitalisation rate at 4 years. A score over 9 (severe bronchiectasis) was associated with 1 year 7.6%–10.5% mortality, and 16.7%–52.6% hospitalisation rate and a 4 year 9.9%–29.2% mortality and 41.2%–80.4% hospitalisation rates. Understanding the factors associated with future morbidity and mortality in bronchiectasis provides a rationale, discussed further elsewhere, for which variables should be assessed and monitored in bronchiectasis.
Good practice point
Consider using the bronchiectasis severity index which may help guide management.
Section 9
Stable state treatment
Airway clearance techniques
Respiratory physiotherapy aims to mobilise secretions and aid effective expectoration, improving airway clearance and providing some control of cough.124 The other aims of respiratory physiotherapy include improving efficiency of ventilation, maintaining or improving exercise tolerance, improving knowledge and understanding, and reducing breathlessness and (thoracic) pain.125 The physiotherapist can discuss step up and step down airways clearance techniques in managing exacerbations. In addition, the respiratory physiotherapist can assist patients who require management of continence issues and musculoskeletal dysfunction.126 In this way, a physiotherapist aims to optimise a patient’s physical function.
Which patients should be taught airway clearance techniques?
A single randomised crossover trial has been published which assesses the efficacy of regular respiratory physiotherapy versus no respiratory physiotherapy in participants with bronchiectasis and chronic sputum expectoration.124 Twenty stable outpatients who did not practice regular respiratory physiotherapy were included. The intervention comprised of twice daily 20–30 min sessions of respiratory physiotherapy using an oscillating positive expiratory pressure device (Acapella Choice) over a 3 month period. There was a significant improvement in all domains and the total Leicester Cough Questionnaire (LCQ) score with regular respiratory physiotherapy (median (IQR) (1.3 (−0.17–3.25) units; P=0.002). It should be noted that the MCID for LCQ is 1.3 units.127 Sputum volume measured over 24 hours increased significantly with regular respiratory physiotherapy (2 (0–6) mL; P=0.02) as did exercise capacity as measured by the incremental shuttle walk test (ISWT) (40 (15-80) m; P=0.001). There was also a significant improvement in quality of life (QoL) with a significant improvement in the St George’s Respiratory Questionnaire (SGRQ) total score (7.77 (−0.99–14.5) unit improvement; P=0.004). No sham treatment was provided in the no respiratory physiotherapy arm and so there is some potential for a placebo effect. However, this study does provide low-quality evidence that regular twice daily respiratory physiotherapy is effective in stable patients.
A consecutive before-after case series assessed the effect of bronchopulmonary hygiene physical therapy (BHPT) on health-related QOL in 53 stable outpatients with bronchiectasis128). BHPT comprised two sessions at least 2 weeks apart and included education and instruction on an appropriate airway clearance technique to be used at home. The LCQ and cough symptom severity visual analogue score (VAS) were administered at initial assessment and more than 4 weeks later. At the follow-up visit, all patients reported administering their BHPT regime at least once per day. After BHPT, there were significant improvements in cough symptoms (mean cough VAS before 43.3 (3.6) vs. after 27.5 (3.1); mean difference 15.8; 95% CI of difference 9.6 to 22; P<0.0001) and cough-related health status (mean LCQ total score before 14.2 vs. after 17.3; mean difference 3.1; 95% CI of difference 2.4 to 3.9; P<0.001). Limitations to the study including the lack of a control group and the use of only subjective outcome measures. In addition, such a variety of components were included as part of BHPT that the efficacy of individual components has not been determined.
Adherence
In an observational, non-comparative study, 75 patients with bronchiectasis and P. aeruginosa were reviewed over a year to determine if baseline beliefs about treatment, clinical factors and QoL predicted adherence.129 41% of patients were adherent to airway clearance. Younger participants and those with a decreased understanding of the necessity of airway clearance were more likely to have reduced adherence.
Evidence statement
Regular twice daily respiratory physiotherapy increases sputum expectoration, improves cough-related health status, quality of life and exercise capacity in individuals with stable bronchiectasis and chronic sputum expectoration (1-)
Bronchopulmonary hygiene therapy (including education and instruction of an appropriate airway clearance technique) at least once per day does lead to an improvement in cough symptoms and cough-related health status in stable outpatients with bronchiectasis (3)
Younger patients (usually considered to be age 50 and under but not limited to this age group) and those with decreased understanding of the necessity of airway clearance may have reduced adherence levels (3)
Recommendation
Teach individuals with bronchiectasis to perform airway clearance. (D)
Good practice points
Airway clearance techniques should be taught by a respiratory physiotherapist.
At initial assessment, a respiratory physiotherapist should educate the patient about their condition and if appropriate give advice on adjuncts (inhaled/oral therapy or exercise) that may enhance effectiveness of their chosen airway clearance technique.
Patients admitted with an exacerbation of bronchiectasis should be seen daily by a respiratory physiotherapist until their airway clearance is optimised.
Which airway clearance techniques should be taught?
There are a number of airway clearance techniques that can be used in the management of bronchiectasis. However, it is beyond the scope of this guideline to describe each airway clearance technique and the reader is referred to detailed descriptions of the techniques for further information.130
In 2002, a survey of the current physiotherapy management of patients with bronchiectasis in the UK found that 91% of senior physiotherapists taught the active cycle of breathing techniques (ACBT) routinely.131 Other techniques such as positive expiratory pressure (PEP), oscillating positive expiratory pressure (OPEP), autogenic drainage (AD) and intermittent positive pressure breathing (IPPB) were used much less frequently.131 Most respondents also used ambulation, exercise and education on the use of inhaled therapy.131
Active cycle of breathing techniques
The active cycle of breathing techniques (ACBT) is the most commonly taught airway clearance technique in patients with bronchiectasis.131 It is often used in conjunction with manual techniques (MTs), postural drainage (PD) or modified postural drainage (MPD). Many of the studies use a combination of ACBT and PD, making evaluation of ACBT alone difficult. A randomised crossover single intervention study by Syed et al compared ACBT to conventional chest physical therapy (CPT).132 Both groups completed 10–15 min of postural drainage (PD) prior to their intervention. ACBT was completed with PD as per ‘evaluation’ (although no details were given on which positions this included) and CPT was completed in PD positions (again no details of these positions) with percussion and shakes completed by the physiotherapist. There were no significant differences in outcomes between the techniques in terms of sputum weight, sputum volume or FEV1 and FVC. Patients however, did find ACBT more comfortable as measured on a visual analogue scale. A number of studies have also shown that when measuring sputum weight, ACBT is as effective as oscillating PEP.133–135 In contrast, a study comparing ACBT to the test of incremental respiratory endurance (TIRE) device found that ACBT (plus PD and vibration) was more effective than the TIRE.136
One study looked at the use of ACBT in an exacerbation.137 Thirty patients with an exacerbation of bronchiectasis were randomly assigned to either ACBT or conventional respiratory physiotherapy (CCPT- diaphragmatic breathing in PD positions with manual techniques). All patients received 14 days of intravenous antibiotics and evaluations were completed at the beginning and end of the admission. The ACBT group had significantly improved measures of the impact of cough on quality of life (Leicester Cough Questionnaire) in both the physical domain of the LCQ (6 v 4 (P=0.023)) and the total LCQ score (14 v 12 (P=0.019)) when compared with CCPT). There were no statistically significant differences between groups in other measures including spirometry and modified MRC dyspnoea scores.
Manual techniques
Manual techniques are among the longest-standing airway clearance techniques and include percussion, shaking, vibrations and over pressure. These techniques are used clinically to both loosen secretions as well as to reduce fatigue or increase effectiveness of other airway clearance techniques.138
A single intervention study (n=22) over 4 days139 looked at the sputum cleared from three different techniques; (1) postural drainage (PD) and coughing (2) PD, percussion and coughing and (3) PD and ‘huffing’. These three techniques were compared with cough technique alone. Techniques were randomly allocated and completed in three 20 min sessions (separated by 10 min rest periods) on the same day. Sputum was collected at baseline, and after each 20 min session at 30 min (session one), 60 min (session two) and 90 min (session three). PD, percussion and coughing cleared more sputum at 60 min (session two) and 90 min (session three) compared with the other techniques. Additionally, PD, percussion and coughing and PD and huffing cleared the most secretions with the worst rheological properties. However, this clearance of the more viscous sputum only occurred when these techniques were performed for two 20 min sessions in succession, indicating a cumulative effect.
Postural drainage
Postural drainage (PD) is the use of gravity-assisted positioning to drain areas of the lung. PD specifically uses gravity to drain the lower and middle lobes using a head down tilt.130
A single treatment of ACBT plus PD was compared with ACBT performed in the sitting position and with the Flutter in the sitting position. The treatment with PD yielded a sputum wet weight twice that of either ACBT in sitting or the Flutter in sitting. Subjects rated their preference for techniques as 44% for the Flutter, 22% for the ACBT in sitting and 33% for the ACBT plus PD. Treatment with PD was associated with significantly more discomfort than the treatments in sitting and was felt to interfere more with daily life than the Flutter and more time consuming.
Many clinicians have concerns about the impact of head-down tilt PD positions on symptoms of gastro-oesophageal reflux disease (GORD). There are no studies assessing the impact of PD on GORD in the bronchiectasis population.
Modified postural drainage
There is no evidence as to whether using mPD does reduce symptoms of GORD or breathlessness in bronchiectasis. There is also no evidence to assess the impact of mPD compared with PD (head down tilt) on the effectiveness of airway clearance.
Positive expiratory pressure
There are no studies formally assessing the effect of positive expiratory pressure (PEP) as an ACT in bronchiectasis. A study evaluated the effect of a single session of PEP therapy in the sitting position on gastro-oesophageal reflux.140 A session of PEP therapy in sitting was not associated with a significant increase in reflux by pH monitoring.
Oscillating PEP
In bronchiectasis, the oscillating PEP (OPEP) devices that have most commonly appeared in the literature to date are the Flutter and Acapella devices, which appear to have similar performance characteristics.141
In a 4 week crossover trial, the Flutter (combined with the Forced Expiratory Technique (FET) and PD as necessary) was shown to be as effective as the ACBT and PD for median weekly sputum weight when used twice daily.133 Neither of the techniques (ACBT or Flutter) had an adverse effect on PEF or breathlessness. Eleven of the 17 subjects expressed a preference for the Flutter.
In a previously described single intervention randomised crossover study comparing Flutter, ACBT and ACBT with PD there were no differences in effectiveness as measured by sputum weight and FEV1 between ACBT and Flutter groups.135 However, although ACBT and PD was the most effective technique in terms of sputum weight, the Flutter was the most preferred by patients (44% preferred Flutter, 22% ACBT and 33% ACBT plus PD).
In a pilot study in Hong Kong, 15 patients with an acute exacerbation of bronchiectasis were randomly allocated to three groups: the Flutter plus deep breathing and coughing (n=5), deep breathing and coughing plus postural drainage (n=5) and deep breathing and coughing alone (n=5).142 There were no differences among the three groups in sputum production or lung function parameters. Patients reported that all techniques were equally easy to use, but again the Flutter was perceived as being the most effective.
A study in 15 stable bronchiectasis patients, looked at outcomes before and after 3 weeks of daily OPEP (Aerobika) use. This showed significant improvements in Patient Evaluation Questionnaire (PEQ)-ease bringing up sputum (P=0.048) and PEQ-global assessment (P=0.01). Ventilation defect percent (VDP) was also evaluated by hyperpolarised MRI, however no significant changes were observed.143
A systematic review evaluated OPEP devices in bronchiectasis.144 In the seven studies reviewed (n=146 patients), OPEP therapy was associated with improvements in sputum expectoration and quality of life measures compared with no treatment. Moreover they concluded that compared with other ACTs, the effects in terms of sputum expectoration, lung function, gas exchange, and symptoms were equivalent. However, the authors did suggest a greater patient preference for oscillating PEP compared with ACBT with or without Gravity Assisted Positioning (GAP).
Autogenic drainage
A randomised crossover study (n=31) in stable bronchiectasis, compared autogenic drainage (AD) to slow expiration with glottis opened in lateral posture (ELTGOL) and temporary positive expiratory pressure (TPEP).145 During physiotherapy sessions, AD and ELTGOL expectorated more sputum than TPEP (AD v TPEP, 3.1 g (95% CI 1.5 to 4.8)). 48.8% of participants stated a preference for AD. The LCQ improved with all techniques, although this did not reach the mean clinically important difference (MCID) for any of the techniques.
Inspiratory muscle training
The test of incremental respiratory endurance is primarily used for inspiratory muscle training. However, it has been proposed as a method of airway clearance in bronchiectasis.136
A randomised crossover pilot study (n=30) compared the effects of a single session of the Acapella (in sitting with huffing included) to a single session of a threshold inspiratory muscle trainer (IMT) (in sitting with huffing included).146 A statistically significant difference was found in sputum volume expectorated with the Acapella treatment (7.16±1.12 mL) compared with IMT (6.46±1.08 mL) with a mean difference of 0.7 mL (P=0.014). Although statistically significant, a difference of 0.7 mL is unlikely to be of any clinical significance. In addition, using a patient preference scale, patients felt that the Acapella was more useful in terms of clearing secretions (P<0.05).
High frequency chest wall oscillation
High frequency chest wall oscillation (HFCWO) is the application of positive pressure air pulses to the chest wall using an inflatable vest. A single randomised controlled trial assessed the effectiveness of HFCWO over a 15 day period. Thirty subjects were randomised into three groups; HFCWO, traditional techniques of respiratory physiotherapy (CPT) (including PEP mask, bottle PEP and oscillating PEP) and a control group (medical therapy only). HFCWO improved breathlessness, quality of life, sputum volume (from 62.5±18.9 mL at admission to 70.0±21.1 in the conventional physiotherapy group and from 52.0±16.9 mL to 72.5±24.0 mL in the HFCWO group). and lung function significantly more than traditional respiratory physiotherapy.
Intrapulmonary percussive ventilation
Intrapulmonary percussive ventilation (IPV) is the delivery of a pulsatile flow of gas to the lungs during inspiration which vibrates the airway walls. A single randomised crossover study (n=22) compared the effectiveness of a single session of IPV in sitting with a single session of chest physical therapy (CPT) in stable bronchiectasis.147 There were no statistically significant differences between groups in the amount of sputum expectorated or dyspnoea score after treatment. There were no adverse events with either treatment that were severe enough to require discontinuation. IPV was associated with less discomfort than CPT.
Intermittent positive pressure breathing
Intermittent positive pressure breathing (IPPB) provides positive pressure throughout inspiration, thereby augmenting tidal volume.148 There is very little evidence investigating the effects of IPPB in bronchiectasis. A single randomised crossover study (n=18) compared the use of IPPB and negative pressure ventilation (NPV) given once per week over a 4 week period.149 Pulmonary function and walking distance did not change significantly after either treatment.
Exercise
A study investigated the impact of an 8 week pulmonary rehabilitation programme.150 The authors suggested a small but significant impact on exacerbation frequency over 12 months in the intervention group (PR) (median 1 (IQR 1–3)) compared with physiotherapy alone (median 2 (IQR 1–3)) (P=0.012).
Evidence statements for airway clearance techniques
The active cycle of breathing techniques is as effective as oscillating positive expiratory pressure (Flutter and Acapella) at clearing sputum. (1-)
The active cycle of breathing techniques plus postural drainage enhances the quantity of sputum expectorated compared with the active cycle of breathing techniques in the sitting position or oscillating positive expiratory pressure (Flutter) in the sitting position. (1-)
The active cycle of breathing techniques (plus postural drainage and vibration) is more effective at clearing sputum than the test of incremental respiratory endurance. (1-)
Oscillating positive expiratory pressure (Acapella) is more effective at clearing sputum than a threshold inspiratory muscle trainer. (1-)
Oscillating positive expiratory pressure (Acapella) improves QoL, sputum volume expectorated and exercise capacity compared with no airway clearance technique over a 3 month period. (1-)
High frequency chest wall oscillation improves breathlessness, quality of life, sputum volume and lung function. (1-)
Recommendations
Offer active cycle of breathing techniques or oscillating positive expiratory pressure to individuals with bronchiectasis. (D)
Consider gravity assisted positioning (where not contraindicated) to enhance the effectiveness of an airway clearance technique. (D)
Good practice points
CT imaging should be reviewed to complement the physiotherapy assessment. Where indicated, this information could be used in order to teach the patient the appropriate postural drainage position(s) for their affected bronchopulmonary segment(s).
Patients should be made aware of the range of available airway clearance techniques.
Consider patient preference and adherence when recommending an airway clearance technique.
Consider the inclusion of the forced expiration technique (huff) should be considered for all airway clearance techniques.
Consider modified postural drainage (no head down tilt) in patients for whom postural drainage is contraindicated or not tolerated.
If symptoms of gastro-oesophageal reflux increase with modified postural drainage (no head down tilt), an airway clearance technique in the sitting position should be taught.
Consider autogenic drainage, positive expiratory pressure, high frequency chest wall oscillation and intrapulmonary percussive ventilation as an alternative airway clearance technique if other techniques are not effective or acceptable to the patient.
Patients should be encouraged to perform regular physical exercise (plus the forced expiration technique/huff) to promote airway clearance.
If there is ongoing haemoptysis, refer back to the respiratory physiotherapist to determine the optimum airways clearance technique.
Evidence statement
Oscillating positive expiratory pressure (Acapella) (plus postural drainage) is effective and safe to use during an acute exacerbation. (1-)
Good practice points
Manual techniques may be offered to enhance sputum clearance when the patient is fatigued or undergoing an exacerbation.
Consider intermittent positive pressure breathing or non-invasive ventilation during an acute exacerbation to offload the work of breathing so fatigued and/or breathless patients can tolerate a longer treatment session and can adopt postural drainage positions.
Research recommendations
Randomised controlled trials using clinically important outcome measures are required to assess the effectiveness of airway clearance techniques in varying severities of bronchiectasis.
Randomised controlled trials are required to evaluate the effects of airway clearance techniques in patients who are undergoing an exacerbation.
How often should patients carry out airway clearance techniques? How long should an airway clearance session last?
Duration
Most clinicians would advocate the use of an airway clearance technique for a period specific to the individual. Commonly, not more than 30 min is recommended. The aim is to perform the airway clearance technique until two clear huffs or coughs are completed. However, this is not always practical in those who are extremely productive. It is important that a balance is found between making sure that the treatment is long enough to maximise airway clearance, but not so long that the patient becomes fatigued.
Frequency
The frequency of the airway clearance technique should be specific to the needs of the individual patient and probably increased during an infective exacerbation. There is no evidence to support a particular frequency with recommendations of once or twice daily treatment commonly given.
Good practice points
The frequency and duration of the airway clearance technique should be tailored to the individual and may alter during periods of exacerbation.
Advise individuals to perform their airway clearance technique for a minimum of 10 minutes (up to a maximum of 30 minutes). After this time they should continue until two clear huffs or coughs are completed, or until the patient is starting to become fatigued.
How soon should the patient be reviewed after the initial assessment?
Initial assessment may take up to an hour, with education and instruction of an appropriate airway clearance technique included. A review of the individual’s ability to effectively carry out this technique should be undertaken within 3 months of this initial appointment.126
Good practice points
Individuals that have been assessed and taught an airway clearance technique should be reviewed by a respiratory physiotherapist within 3 months of their initial assessment.
Individuals with bronchiectasis who are followed up in secondary care should be assessed by a respiratory physiotherapist as part of their annual clinical review to ensure their airway clearance regimen is optimised.
All individuals with a deterioration in their condition (increased frequency of exacerbations and/or worsening of symptoms) should have their airway clearance technique reviewed by a respiratory physiotherapist (See figure 1 – management of the deteriorating patient).
Mucoactives in bronchiectasis
Mucoactive medications describe medications which may have a direct impact on the clearance of mucus from airways. These can be defined by their different methods of action including expectorants (aid and/or induce cough), mucolytics (thin mucus), mucokinetics (facilitate cough transportability), and mucoregulators (suppress mechanisms underlying chronic mucus hyper secretion, such as glucocorticosteroids). Bronchiectasis research has mainly focused on mucolytics (DNase),151 152 mucokinetics/expectorants (humidification, normal/isotonic saline (0.9% saline) (IS), hypertonic saline (3% saline and above) (HS)153–158 and mannitol159 160 and there is a small amount of evidence in mucoregulators (erdosteine)161 and bromhexine.162
Humidification
A small study (n=7) showed that 30 min of cold water, jet nebulising humidification via a facemask before respiratory physiotherapy (postural drainage and the forced expiration technique) significantly increased sputum yield and radio aerosol clearance compared with respiratory physiotherapy alone.154 A further study (n=10) using warm air humidification for 3 hours a day also showed a significant increase in radiolabelled clearance in the treatment group compared with the control group.163
Saline
A small single study (n=8) found that the use of nebulised IS immediately before respiratory physiotherapy (postural drainage and the forced expiration technique) yielded significantly more sputum than physiotherapy alone.153
A four way single intervention crossover study looking at ACBT alone, ACBT and terbutaline, ACBT and isotonic saline (IS) and ACBT and hypertonic saline (HS), suggested that HS gave an additional improvement to QoL, FEV1, sputum weight, ease of expectoration and viscosity in addition to the benefit shown by IS over that of terbutaline or ACBT alone.158
A 4 week crossover study in 32 patients with bronchiectasis compared 7% HS to a placebo (IS). FEV1 improved in the HS group compared with the IS group by 15.1 (1.8)% (P<0.01); FVC by 11.2 (0.7)% (P<0.01), QoL as measured by SGRQ showed an improvement of 6 units (P<0.05) in the HS group.155 Moreover sputum viscosity (subjective pourability), ease of clearance (as measured by a visual analogue scale) and healthcare utilisation also all improved in the HS group compared with IS.
A long term study (12 months) of 40 participants was designed to investigate the impact of HS compared with IS when used with ACBT, demonstrated that both IS and HS saline had a positive impact on all domains of the SGRQ and the LCQ after three, six and 12 months, and on FEV1, with an improvement in the IS group of (mean) 90 mL (11 to 169); P=0.04 compared with baseline.157
In summary this evidence suggests that HS may improve QoL outcomes and sputum clearance in individuals with bronchiectasis, however it is unclear if this benefit is over and above that of IS.
Mannitol
Many studies have suggested an in vitro benefit of mannitol164 and have shown it to be tolerated in inhaled devices by individuals with bronchiectasis in feasibility studies.165 In a phase three study of 343 subjects with bronchiectasis,159 subjects were randomised into either placebo (40 mg mannitol) versus treatment dose mannitol (340 mg) over a 12 week intervention period. An improvement was seen in SGRQ in the mannitol group, however this was not a clinically significant change. A subgroup of participants (n=123) who continued to a further 52 weeks open label study continuing on mannitol had a reduction in sputum plugging on CT scan. In a large phase 3 RCT in 461 patients with bronchiectasis over 12 months,160 randomised patients received either placebo (low dose mannitol) or mannitol (400 mg) over 12 months. No differences were seen in the primary end point of exacerbation frequency between the two groups at these time points. However, this study did show a prolongation in time to first exacerbation and a small improvement in quality of life in the mannitol group.
In view of the potential for bronchoconstriction, a challenge test with hyperosmolar agents is suggested. All included studies performed a challenge test to assess for bronchoconstriction and/or bronchial hyper-reactivity prior to use of the device/medication.155–160 Those individuals who reported chest tightness, wheeze, and difficulty in breathing or had a 10% or 15% reduction in spirometry were withdrawn from the studies. All the studies suggested that such events were minimal thereby showing good tolerance of hypertonic saline and mannitol. The studies varied on the use of a pre dose bronchodilator. However clinical practice suggests that pre-treatment with a bronchodilator may be necessary for those with the potential for bronchial hyper-reactivity (eg, a diagnosis of asthma, or defined bronchodilator reversibility).
Mucolytics
Recombinant human DNase (DNase, dornase alpha, Pulmozyme) breaks down the DNA released at the site of infection by the neutrophils. DNA causes the sputum to become thick and tenacious and therefore inhaled DNase makes the sputum less viscid and therefore easier to expectorate. A multi-centre study in 349 patients with idiopathic bronchiectasis randomised patients to use either 2.5 mg DNase versus a placebo.152 There was a significant increase in the rate of both protocol-defined exacerbations (0.66 rate of exacerbations per patient per 166 days compared with 0.56 rate for those in placebo group, relative risk=1.17) as well as an increase in non-protocol defined exacerbations (relative risk 2.01) within the DNase group. DNase had a small but negative effect on FEV1 (−3.6% in DNase v 1.7% in control, P=0.05)
There have been very few trials reviewing the use of oral mucolytics in bronchiectasis. One study (n=88) reviewed the addition of bromhexine hydrochloride to an antibiotic during an acute infective exacerbation compared with a placebo.162 It is thought this medication may influence sputum clearance by increasing the production of serous mucus thereby making the sputum thinner and less viscous. Results suggest that this medication was effective, as the percentage change in sputum production was greater in the bromhexine group at 7, 10 and 16 days (mean difference (MD) −21.5 mL, 95% CI −38.9 to −4.1 at day 16). Moreover the difficulty in expectoration was also improved in the bromhexine group at day 10 (MD −0.53, 95% CI −0.81 to −0.25) however it had no impact on FEV1.Bromhexine hydrochloride is not widely available in the UK and is not listed in the BNF.
Erdosteine is another mucolytic which is thought to modulate mucus production through the scavenging activity of free radicals. A study in 2007 compared the use of erdosteine and respiratory physiotherapy to respiratory physiotherapy alone over a 15 day period in a bronchiectasis population (n=30).161 This study was small and of poor methodological quality due to limited control of bias. Small changes were seen in some subjective sputum characteristics and FEV1 in the erdosteine group.
In the UK from National Audits 2010 and 2011, Carbocysteine was commonly prescribed (27%–30%).166 There are no randomised controlled trials to demonstrate benefit.
Evidence statements
Recombinant human DNase increases exacerbation frequency in bronchiectasis. (1+)
Isotonic and hypertonic saline can improve cough related quality of life QoL and health related quality of life (HQoL) in patients with bronchiectasis in addition to airway clearance. (1-)
Mannitol did not improve exacerbation frequency but was shown to increase the time to first exacerbation, demonstrated a small improvement in QoL and may reduce sputum plugging. (1+)
The use of humidification prior to airway clearance improves sputum yield and radiolabeled clearance, when used in short term interventions (>1 month). (3)
Oral mucolytics can improve sputum expectoration. (1-)
Recommendations
Do not routinely use recombinant human DNase in adults with bronchiectasis. (A)
Consider the use of humidification with sterile water or normal saline to facilitate airway clearance. (D)
Good practice points
Consider a trial of mucoactive treatment in patients with bronchiectasis who have difficulty in sputum expectoration.
Perform an airway reactivity challenge test when inhaled mucoactive treatment is first administered.
Consider pre-treatment with a bronchodilator prior to inhaled or nebulised mucoactive treatments especially in individuals where bronchoconstriction is likely (patients with asthma or bronchial hyper-reactivity and those with severe airflow obstruction FEV1 <1 litre).
If carbocysteine is prescribed, a 6 month trial should be given and continued if there is ongoing clinical benefit.
See appendix 2: Challenge test details
Research recommendation
Randomised controlled trials are needed to assess the long term impact of muco-active therapies.
What is the evidence for long term anti-inflammatory therapies in bronchiectasis?
Airway inflammation is dominated by neutrophils although there is evidence to implicate multiple other inflammatory cells and pathways in the pathophysiology of bronchiectasis.167 168
Inhaled corticosteroids (ICS)
In bronchiectasis, a systematic review conducted in 2009 identified six single centre randomised controlled trials.169 Two studies were crossover studies170 171 while the other four were parallel group studies.172–175 All were double blind placebo controlled studies with the exception of Martinez et al 2006 which was open label.172 Studies used multiple difference steroid preparations and doses (beclomethasone 800 μg/day, 1500 μg, fluticasone 500 μg/day and 1000 μg/day). Study duration ranged from 4 to 6 weeks to 6 months. Two studies reported reductions in sputum volume with ICS treatment.170 172 A small improvement in lung function was suggested by the meta-analysis (90 mL for FEV1 and FVC) in studies of ≤6 months but this was not statistically significant if the study that was not placebo controlled was removed.169 No reduction in exacerbations was identified. In longer term studies (>6 months) no significant improvement in lung function or exacerbations were identified.169 The BTS guideline development group identified no new randomised controlled trials since 2009.
Clinically important adverse events associated with inhaled corticosteroids have been identified. Holme et al identified a high frequency of adrenal suppression associated with ICS treatment in bronchiectasis.176 A statistically significant increase in adverse effects was reported for high dose ICS in the trial of Martinez et al (P=0.04).172 A trial of high dose budesonide vs budesonide with formoterol identified a numerical increase in the frequency of local side effects with high dose ICS (pharyngeal irritation, dysphonia and gingivitis) and a single case of pneumonia which is a recognised adverse effect of inhaled corticosteroid treatment in COPD.177
Oral corticosteroids
No randomised controlled trials of oral corticosteroids either when stable or during exacerbations could be identified.178 No observational data were identified.
Phosphodiesterase four inhibitors (PDE4 inhibitors)
There are no randomised trials of PDE4 inhibitors in bronchiectasis. In addition, no observational data were identified.
Methylxanthines
No randomised controlled trials were identified in bronchiectasis for these drugs.179 No observational data were identified.
Indomethacin
A single trial of 25 adults with chronic lung diseases that included patients with bronchiectasis was identified. This study showed a significant reduction in sputum production over 14 days in patients that received inhaled indomethacin compared with placebo (difference −75 g/day 95% CI −134.6 to −15.4).180 There were also significant improvements in dyspnoea. No further large trials have been performed.
Leukotriene receptor antagonists
No randomised trials or observational studies of leukotriene receptor antagonists in bronchiectasis have been performed.181
Neutrophil elastase inhibitors
Neutrophil elastase is a proteolytic enzyme released by neutrophils which may have a role in disease progression.182 A single randomised controlled trial of 38 patients treated with a neutrophil elastase inhibitor for 4 weeks compared with placebo (n=16) was identified. The study found no difference in sputum neutrophils but an improvement of 100 mL in the FEV1 in the NE inhibitor group (P=0.006).183 No larger trials have yet been performed.
CXCR2 inhibitors
A double blind randomised placebo-controlled trial of the CXCR2 antagonist AZD5069 in bronchiectasis for 28 days recruited 52 patients with a primary outcome of sputum neutrophil counts. This study showed a significant reduction in absolute neutrophil counts (69% vs placebo, P=0.004). There was no significant difference in exacerbations or other clinical outcomes. Some sputum inflammatory markers e.g IL-6, GRO-α, IL-1β and IL-8 increased with AZD5069 vs placebo. Four patients discontinued therapy in the active group vs 0 in the placebo group.184
Statins
Statins have multiple anti-inflammatory and immunodulatory effects in addition to their effects on cholesterol. A randomised placebo controlled trial has been performed in bronchiectasis. 60 patients were treated with atorvastatin 80 mg daily for 6 months (n=30) vs. placebo (n=30).185 The primary endpoint was improvement in cough assessed by the Leicester Cough Questionnaire. The change from baseline to 6 months in LCQ score differed between groups, with a mean change of 1.5 units in patients allocated atorvastatin versus –0.7 units in those assigned placebo (mean difference 2.2, 95% CI 0.5–3.9; P=0.01). 12 (40%) of 30 patients in the atorvastatin group improved by 1.3 units or more on the LCQ compared with five (17%) of 30 in the placebo group (difference 23%, 95% CI 1–45; P=0.04). Ten (33%) patients assigned atorvastatin had an adverse event versus three (10%) allocated placebo (difference 23%, 95% CI 3–43; P=0.02).185 No larger trials have been performed.
A randomised placebo cross-over trial investigated atorvastatin 80 mg daily for 3 months in patients chronically infected with P. aeruginosa. Statin therapy did not improve the primary endpoint for improved cough assessed by the Leicester Cough Questionnaire. There were however significant improvements in the St. George’s Respiratory Questionnaire (5.6 Unit improvement) and a reduction in serum CXCL8, TNFα and ICAM-1 in the statin treated group.186
Evidence statements
Inhaled corticosteroids may reduce sputum volume in bronchiectasis but are associated with adverse events including local and systemic effects. (1+)
There was insufficient evidence to evaluate the role of oral corticosteroids, PDE4 inhibitors, methylxanthines or leukotriene receptor antagonists in bronchiectasis. (4)
A small trial of inhaled indomethacin which included some patients with bronchiectasis showed reduced sputum volume and improved dyspnoea. (1-)
A small randomised trial of oral neutrophil elastase inhibitors in bronchiectasis showed improved FEV1 but no other benefits. (1-)
A small trial of CXCR2 antagonists showed reduced sputum neutrophil counts but no clinical benefits. (1-)
A small randomised trial of statins in bronchiectasis showed improved cough, but an increase in adverse events. (1-)
A small randomised trial of statins in bronchiectasis chronically infected with P. aeruginosa showed improved health related quality of life. (1-)
Recommendations
Do not routinely offer inhaled corticosteroids to patients with bronchiectasis without other indications (such as ABPA, chronic asthma, COPD and inflammatory bowel disease). (B)
Do not offer long-term oral corticosteroids for patients with bronchiectasis without other indications (such as ABPA, chronic asthma, COPD, inflammatory bowel disease). (D)
Do not routinely offer PDE4 inhibitors, methylxanthines or leukotriene receptor antagonists for bronchiectasis treatment. (D)
Do not routinely offer CXCR2 antagonists, neutrophil elastase inhibitors or statins for bronchiectasis treatment. (B)
Good practice point
Inhaled corticosteroids have an established role in the management of asthma and a proportion of patients with COPD which are common co-morbid conditions in bronchiectasis.
Research recommendation
Randomised controlled trials are needed to assess the long term impact of anti-inflammatory therapies.
What treatments improve outcomes for patients with stable bronchiectasis?
Long term antibiotic treatment (>=3 months)
Oral antibiotics
Several randomised controlled studies have been performed to ascertain the effect of long term antibiotics in bronchiectasis. Some of the earliest were performed in the 1950s and so the diagnostic techniques defining the patient population (bronchiectasis and aetiology), outcome measures, statistical analysis and trial conduct are suboptimal by contemporary standards. The MRC study published in 1957 involved 122 bronchiectasis patients from seven centres randomised to receive penicillin 500 mg four times a day or oxytetracycline 500 mg four times a day or identical placebo two capsules four times a day, for 2 days per week for 1 year.187 No power calculation or formal statistical analysis was performed and no qualitative or quantitative sputum microbiology was performed. Oxytetracycline appeared most efficacious with least exacerbations requiring rescue antibiotics, a 50% reduction in sputum purulence, markedly less days confined to bed and less days off work. Treatment with penicillin appeared to be associated with a marginal treatment response compared with placebo. A study by Cherniack et al published in 1959 involved 67 patients (45 with bronchiectasis) from a single centre.188 Patients were randomised to receive tetracycline (2 g/day), Penicillin G (1,600,000 units/day) Oleandomycin-Penicillin (2 g/day) or identical placebo. In a subgroup analysis involving only patients with proven bronchiectasis, there were no statistically significant differences between the treatment groups but this may reflect a lack of power.188 A further study in 38 bronchiectasis patients looked at the use of daily oral amoxicillin 3 g bd over 32 weeks. In this study CTs were not performed and no reduction in exacerbations was demonstrated, but some improvement in sputum volume, diary card symptom improvement and less time away from work.189 These studies suggest that tetracycline based regimens may reduce exacerbation frequency, duration of illness and improve symptoms in patients with bronchiectasis, with penicillin based regimens being less effective.
Recent longer term antibiotic trials have only enrolled patients with bronchiectasis confirmed by high resolution CT scans. The primary clinical endpoints have concentrated on exacerbation burden with either time to next exacerbation or exacerbation frequency. There have been three recent, high quality (although small studies and heterogeneous design) RCTs performed comparing a macrolide antibiotic to placebo given over 6–12 months.
Macrolides
Wong et al studied 500 mg three times weekly azithromycin for 6 months in 141 patients,190 Altenburg et al azithromycin 250 mg od for 1 year in 83 patients,191 and Serisier et al 250 mg bd erythromycin for 48 weeks in 117 patients.192 Each study used different entry criteria: 71/141 in the Wong study did not culture pathogens at baseline, and 17 cultured P. aeruginosa190 ; Altenburg required at least one pathogen cultured from sputum in the previous year and 12/83 had P. aeruginosa191 ; Serisier stratified for P. aeruginosa at baseline and had a relatively high (41/117) number of patients with this pathogen that is associated with more severe disease.192 Wong et al required at least one exacerbation, Serisier et al at least 2, and Altenburg et al at least 3.190–192
In fact patients had a wide variation in the number of exacerbations in the previous year, but on average more than these entry criteria: Wong et al 3–4190 and Altenburg et al 4-5.191 All three studies showed a significant reduction in exacerbation frequency: Wong et al 0.59 exacerbations per patient with azithromycin cf 1.57 with placebo P<0.0001190; Altenburg et al median number of exacerbations 0 with azithromycin cf two with placebo P<0001, which is 0.84 per patient with azithromycin cf 2.05 with placebo191; Serisier et al 1.29 per patient with erythromycin cf 1.97 with placebo P=0.003.192There have been four meta-analyses which have all included these three studies together with shorter studies and/or paediatric studies.193–196 The following consistent findings have been: a reduction in the number of patients who had at least one exacerbation (RR 0.55–0.7); small improvements in FEV1 occurred in 2 of the three trials and was confirmed in the meta analyses; the benefit was not dependent on microbiology; quality of life results were more variable Wu et al196 2014 in the five trials included in the meta analysis that used SGRQ a 5.4 fall in total score P=0.02,196 but in the Guang-Ying195 2014 meta analysis that included three studies which used SGRQ the changes were not significant195); there were no significant increase in adverse events with macrolide, but GI side effects increase on macrolide (low dose erythromycin better tolerated than azithromycin), but in most cases not sufficient to lead to withdrawal; increased macrolide resistance occurs which was best studied by Serisier et al 2013 which showed a 27.7% increase on oropharyngeal streptococci resistance with erythromycin compared with 0.04% with placebo P<0.001.192
The results were variable at follow-up after treatment stopped, Wong suggests benefit maintained in 6 months after cessation,190 Altenburg that it is lost (in terms of exacerbations).191 Wong found treatment effects significantly greater in patients with higher SGRQ scores.190 There is some evidence favouring azithromycin. The Guang Ying et al meta analysis showed that on subgroup analysis azithromycin demonstrated lower exacerbation frequency whereas erythromycin did not.195 In addition, the benefit of erythromycin compared with placebo was more delayed in the erythromycin study compared with the other two azithromycin studies. The latter observation may however be accounted for by the higher proportion of P. aeruginosa patients in this study.
A further analysis by 16S RNA gene sequencing of paired sputum samples, baseline and end of treatment, from the BLESS trial showed a reduced abundance of H. influenzae, and an increased relative abundance of P. aeruginosa, in patients treated with erythromycin without P. aeruginosa at the start of the trial.192 This was not shown by routine bacteriology, but raises a concern which requires further investigation.197
Inhaled/nebulised antibiotics
In addition to the use of long term oral antibiotics, there have been several studies assessing the efficacy of long term inhaled antibiotics in bronchiectasis. Several of these have provided proof of concept data demonstrating a reduction in bacterial counts, usually at the 28 day time point.198 199 Haworth et al studied 144 bronchiectasis patients with chronic pseudomonas infection treated with Promixin (colistin) or 0.45% saline who were followed up until the first exacerbation or 6 months.200 Although the study did not reach significance in its primary endpoint of time to next exacerbation (165 days vs 111 days P=0.11), this was significant in a predetermined ‘compliant’ population (those that took the medication for>=80% of the time (168 vs 103 days P=0.028)). This could be accurately defined because of an electronic chip on the nebuliser. In the whole group analysis they also demonstrated a significant reduction in P. aeruginosa colony forming unit (CFU) count at 12 weeks and a significant improvement in the SGRQ total score at 26 weeks. There was no difference in FEV1, sputum weight or adverse events. The incidence of adverse effects leading to discontinuation was low and similar in both groups.
A similar increase in time to next exacerbation was also seen in the per protocol population of a small phase 2 study of 42 bronchiectasis patients with P. aeruginosa with three on/off cycles of dual release inhaled ciprofloxacin. In this study, the median time to exacerbation was 134 vs 58 days (P=0.057 modified intention to treat, 0.046 per protocol).199
Time to next exacerbation was also extended with the use of inhaled gentamicin (80 mg bd) compared with normal saline control in a 65 patient RCT with patients who had potentially pathogenic micro-organisms, who were treated for 1 year with a 3 month follow-up (61.5 vs 120 days P=0.02) and the exacerbation number was also reduced in the active group (0 (0–1) vs 1.5 (1–2) p<0.0001).201 Quality of life measures improved, sputum became less purulent and exercise capacity increased. Emergence of resistance did not occur, however benefits were lost quickly on stopping treatment during the 3 month follow-up. In this study patients were not masked to intervention. Although 7/32 patients in the gentamicin arm reported bronchoconstriction, this only led to withdrawal in two patients (the same as the saline arm). Further analysis of this study also documented reductions in sputum inflammatory markers (including myeloperoxidase activity, neutrophil elastase, interleukin-8 and tumour necrosis factor-alpha).168
Barker and colleagues conducted two large double blinded multi-centre trials (AIR-BX1 (n=266) and AIR-BX2 (n=274)) administering inhaled aztreonam 75 mg (aztreonam for inhalation solution or AZLI) or placebo for two 4 week periods followed by a 4 week washout period after each.202 The primary end point which was change in QOL-B respiratory symptom scores (RSS) from baseline to 4 weeks was not attained in either of the studies. The secondary end points were change in QOL-B-RSS from baseline to week 12 and time to first protocol defined exacerbation to week 16. Although the QOL-B-RSS numerically increased in all groups in both studies at week 4 and week 12, the mean change from baseline was only statistically significant in week four in the AIR-BX2 study alone. However, this change of 4.6 points although statistically significant was not clinically significant as the minimal important difference for the QOL-B-RSS is 8.0 points. The median time to first protocol defined exacerbation was reached in only the placebo group in AIR-BX1. In the AZLI treated group there were more treatment related adverse events necessitating patients to drop out. In summary, although this is a large multi centred RCT with aztreonam, there were perhaps some inherent faults with the design of the study, notably the heterogeneity of the cohorts in the study. AZLI treatment was not associated with significant clinical benefit in bronchiectasis as measured by the QOL-B-RSS and time to next exacerbation.
Most recently, Ciprofloxacin (32.5 mg) dry powder for inhalation (DPI) twice-daily was studied in two large (RESPIRE 1 n=416 and RESPIRE 2 n=521) randomised, double-blind, placebo-controlled (two active:1 placebo) trials.203 204 A novel aspect of the studies was that 14- or 28 day on/off cycles were compared for 48 weeks. Patients had a documented history of two or more exacerbations in the previous year and had positive sputum cultures for a pathogenic species at screening. The primary end points were time to first exacerbation and frequency of exacerbations. Patients had to meet a strict definition of an exacerbation during the trial, and the number occurring were low (42.8% in RESPIRE 1% and 58% in RESPIRE 2 of placebo patients did not have an exacerbation). In RESPIRE one ciprofloxacin DPI 14 day on/off significantly delayed time to first exacerbation versus pooled placebo (median time >336 days versus 186 days, HR 0.53, 97.5% CI 0.36 to 0.80, P=0.0005) and reduced frequency of exacerbations versus matched placebo by 39% over 48 weeks (mean number of exacerbations 0.6 vs 1.0, incidence rate ratio 0.61, 97.5% CI 0.40 to 0.91 P=0.0061). The 28 day on/off cycle results were not significant, and in RESPIRE 2, neither on/off cycle met the primary end points, although there were positive trends. A liposomal ciprofloxacin preparation for inhalation has also been studied with the complete results not published at the time of writing. The pooled results of the RESPIRE studies suggest a positive signal for response to inhaled ciprofloxacin, but the drug has not been granted marketing authorisation. Future trials must include patients more likely to exacerbate.
Intravenous antibiotics
A small study assessing the impact of cyclical 8 weekly intravenous antibiotics has also been performed in 19 patients with five or more bronchiectasis exacerbations and ill health between antibiotic courses, both defined subjectively.205 Antibiotic courses were based on sputum sensitivity. The majority of patients were not on other long term antibiotics at entry to the study (16/19). This approach demonstrated a small, statistically significant reduction in exacerbations (9.3 to 8) and hospital bed days (43.1 to 19.4), and improvement in incremental shuttle walk test with a proportion of patients experiencing improved health questionnaire status. However the study was subject to recall bias and the positive health effects of being in a study and having regular follow-up. There were two meta analyses done to assess the efficacy of long term antibiotics (>4 weeks in bronchiectasis). While Hnin et al looked at long term antibiotics irrespective of route of delivery,206 Yang et al assessed long term inhaled antibiotics only.207 18 studies involving 1157 patients met the inclusion criteria in the metaanalysis conducted by Hnin et al. Based on the number of participants with at least one exacerbation, the meta-analysis showed significant effects in favour of the intervention (OR 0.31, 95% CI 0.19 to 0.52; P value <0.00001), with events occurring in 271 per 1000 people in the intervention arm (95% CI 126 to 385) and in 546 per 1000 in the control population, based on evidence of moderate quality. A non-statistically significant reduction in hospitalisation favoured the use of prolonged antibiotics with a moderate quality grade of supporting evidence (37 per 1000 in the intervention arm (95% CI 13 to 96) and 87 per 1000 in control (OR 0.40, 95% CI 0.14 to 1.11; P value =0.08). Drug resistance developed in 36 of 220 participants taking antibiotics compared with 10 of 211 participants given placebo or standard therapy (OR 3.48, 95% CI 1.20 to 10.07; P value =0.02), thereby translating to natural frequencies of 155 per 1000 in the intervention arm (95% CI 59 to 346) and 50 per 1000 in the control arm. The intervention was well tolerated with no overall significant difference in withdrawal between treatment and placebo groups (OR 0.91, 95% CI 0.56 to 1.49). Diarrhoea was commonly reported as an adverse event, particularly with an oral intervention.
The authors concluded that the available evidence shows benefit with use of prolonged antibiotics, at least halving the odds of exacerbation (with 275 fewer exacerbations per every 1000 people treated in the antibiotic arm compared with the control arm) and hospitalisation (50 fewer hospitalisations per 1000 people in the antibiotic arm compared with the control arm). However, the risk of emerging drug resistance was increased more than threefold.
Eight randomised controlled trials recruiting 539 patients were included in the meta-analysis by Yang et al.207 Long-term inhaled antibiotics showed a reduction of the sputum bacterial density (weighted mean difference=2.85, 95% CI: 1.6 to 4.09, P<0.00001) and augmented eradication of sputum P. aeruginosa (OR=6.6, 95% CI: 2.93 to 14.86, P<0.00001). No studies showed higher risk of P. aeruginosa resistance after inhaled therapy. In addition, nebulized therapy reduced the amount of patients with exacerbation (OR=0.46, 95% CI: 0.21 to 1.00, P=0.05). However, patients with inhaled antibiotics were more likely to suffer wheeze (OR=6.74, 95% CI: 2.22 to 20.52, P=0.0008) and bronchospasm (OR=2.84, 95% CI: 1.11 to 7.25, P=0.03). The authors concluded that long-term inhaled antibiotics can effectively reduce the sputum bacterial density, increase P. aeruginosa eradication and attenuate the risk of exacerbation, accompanied however by higher risk of wheeze and bronchospasm.
Evidence statements
Long term antibiotics reduce exacerbations in bronchiectasis. (1++)
Inhaled colistin 1 MU twice daily delivered through the I-neb improves quality of life in bronchiectasis patients with chronic P. aeruginosa infection and one or more exacerbations per year. (1+)
Inhaled colistin 1 MU twice daily delivered through the I-neb extends the time to exacerbation in treatment compliant bronchiectasis patients with chronic P. aeruginosa infection and one or more exacerbations per year. (1+)
Inhaled gentamicin increases the time to exacerbation, reduces exacerbation rate and improves quality of life in patients with bronchiectasis with chronic infection with a potentially pathogenic micro-organism and two or more exacerbations per year. (1+)
Azithromycin and erythromycin reduce exacerbation number, and the number of patients that had at least one exacerbation, in patients with bronchiectasis. (1++)
Tetracyclines may reduce exacerbation number in patients with bronchiectasis. (2+)
Patients recruited into the long term antibiotic RCTs had more (≥3) exacerbations in the preceding year than defined by the inclusion criteria. (1+)
Inhaled aztreonam twice daily for 4 weeks is not associated with clinically significant benefit as measured by changes in the QOL-B-RSS and time to first exacerbation. Additionally, aztreonam has a higher incidence of treatment related adverse events and discontinuation secondary to adverse events. (1+)
Cyclical intravenous antibiotics may reduce exacerbation number and hospital bed days in patients with ≥5 exacerbations and subjective ill health between exacerbations. (3)
Recommendations
Consider long term antibiotics in patients with bronchiectasis who experience three or more exacerbations per year. (A)
In these patients, the following are recommended (see figure 2 and appendix 2 and 3)
P. aeruginosa colonised patients
Use inhaled colistin for patients with bronchiectasis and chronic P. aeruginosa infection. (B)
Consider inhaled gentamicin as a second line alternative to colistin for patients with bronchiectasis and chronic P. aeruginosa infection. (B)
Consider azithromycin or erythromycin as an alternative (eg, if a patient does not tolerate inhaled antibiotics) to an inhaled antibiotic for patients with bronchiectasis and chronic P. aeruginosa infection. (B)
Consider azithromycin or erythromycin as an additive treatment to an inhaled antibiotic for patients with bronchiectasis and chronic P. aeruginosa infection who have a high exacerbation frequency. (D)
Non- P. aeruginosa colonised patients
e. Use azithromycin or erythromycin for patient with bronchiectasis. (A)
f. Consider inhaled gentamicin as a second line alternative to azithromycin or erythromycin. (B)
g. Consider doxycycline as an alternative in patients intolerant of macrolides or in whom they are ineffective. (C)
Good practice points
Antimicrobial stewardship is important
Prior to starting long term macrolides, for safety reasons: 1) ensure no active NTM infection with at least one negative respiratory NTM culture; 2) use with caution if the patient has significant hearing loss needing hearing aids or significant balance issues.
Prior to starting long term inhaled aminoglycosides, for safety reasons: 1) avoid using if creatinine clearance <30 mL/min; 2) use with caution if the patient has significant hearing loss needing hearing aids or significant balance issues; 3) avoid concomitant nephrotoxic medications.
Counsel patients about potential major side effects with long term antibiotics, and to seek urgent attention if these develop.
Review the patient’s culture and mycobacterial status, optimise airway clearance and treat other associated conditions before starting long term antibiotics.
Prophylactic antibiotics should be only started by respiratory specialists.
Review patients on long term antibiotics 6 monthly with assessment of efficacy, toxicity and continuing need. Monitor sputum culture and sensitivity regularly, although in vitro resistance may not affect clinical efficacy.
As adverse event frequency of azithromycin is likely to be dose related, 250 mg 3 x/week is a pragmatic starting dose which can then be increased according to clinical response and adverse events.
Thresholds for long term treatment may reduce if the patient is symptomatic between exacerbations and/or the exacerbations respond poorly to treatment and/or the patient is at high risk of severe exacerbation for example, immunosuppressed.
Long term antibiotic choice is complex and has to take into account factors such as tolerance, allergies and sensitivity, therefore in some circumstances, other long term antibiotic regimens may be appropriate (see appendix 3).
Perform a suitable challenge test when stable before starting inhaled antibiotics (see appendix 2)
Consider cyclical IV antibiotics in patients with repeated infections (≥5/year) despite other treatments.
Alternative inhaled/nebulised agents may become licensed as international studies are completed.
For patients receiving long term prophylactic oral antibiotics, the preferred option is to remain on the same antibiotic as opposed to monthly rotation of antibiotics. If there is a subsequent lack of efficacy, the antibiotic can be changed guided by sensitivity results.
Research recommendation
Long term randomised controlled trials of oral and inhaled antibiotics are needed to assess their efficacy and safety in patients with bronchiectasis who have frequent respiratory tract infections with recurrent P. aeruginosa infection or other potential pathogenic micro-organisms.
Does long term bronchodilator treatment improve outcomes for patients with bronchiectasis?
Patients with bronchiectasis frequently have airflow obstruction and more than 60% of bronchiectasis patients have daily symptoms of breathlessness.120 There is limited supporting evidence for the use of bronchodilators, although both beta-2-agonists and anticholinergic bronchodilators are commonly used in clinical practice.166
Long acting Beta-2-agonists
A systematic review published in 2014 identified only one eligible randomised controlled trial of long acting beta-2-agonists.208 This included 40 patients with a primary outcome of health related quality of life. It indicated improved quality of life with the use of budesonide/formoterol versus budesonide alone. The Cochrane review identified significant methodological issues with this trial including inadequate and incorrectly reported blinding and inadequate reporting of the data.208
Long acting anticholinergic agents
There are no randomised controlled trials of long acting muscarinic antagonists in bronchiectasis.209 Although studies suggest that some patients with bronchiectasis will have significant reversibility to anti-cholinergic bronchodilators, there is no evidence to establish that reversibility is a requirement for benefit.210
Short acting bronchodilators
There are no randomised controlled trials to demonstrate if short acting bronchodilators are beneficial in bronchiectasis.211
As there are no large randomised controlled trials of bronchodilators in bronchiectasis there are limited data on the safety of these agents. Data from COPD and asthma, however, suggests that they have an acceptable safety profile.
Evidence statement
Long acting beta-2-agonists may be beneficial in patients with symptoms of breathlessness. (4)
Long acting anti-cholinergics in bronchiectasis may be beneficial in patients with symptoms of breathlessness. (4)
No evidence was identified to support the use of short acting beta-2-agonists. (4)
Bronchodilator treatment may include short or long acting beta-agonists, short or long acting anti-cholinergic bronchodilators, or combined bronchodilators. There is no evidence to guide which of these is the optimal strategy in bronchiectasis (4)
Recommendations
Use of bronchodilators in patients with bronchiectasis and co-existing COPD or asthma should follow the guideline recommendations for COPD or asthma. (D)
Offer a trial of long acting bronchodilator therapy in patients with symptoms of significant breathlessness. (D)
Reversibility testing to beta-2-agonists or anticholinergic bronchodilators may help to identify patients with co-existing asthma but there is no evidence to suggest that a response is required in order to benefit from bronchodilators. (D)
Pulmonary rehabilitation
Evidence summary
A recent cross-sectional study by Bradley et al assessed the physical activity of participants with bronchiectasis (n-=63).212 Only 11% of participants met the recommended physical activity guidelines of ≥150 min of at least moderate activity per week.213 There are four randomised controlled trials (RCTs) which investigate the effects of pulmonary rehabilitation (PR) in bronchiectasis.150 214–216 Mandal et al (2012) conducted a pilot RCT (n=30) comparing an 8 week PR programme plus respiratory physiotherapy with respiratory physiotherapy alone.215 Respiratory physiotherapy was carried out twice daily using the oscillatory positive expiratory pressure (PEP) device the Acapella Choice. Outcome measures were the incremental shuttle walk test (ISWT), the endurance shuttle walk test (ESWT), the Leicester Cough Questionnaire (LCQ) and the St George’s Respiratory Questionnaire (SGRQ). After 8 weeks there was a significant improvement in all outcome measures in the intervention group compared with the control group. The mean difference in the ISWT, LCQ and SGRQ were all clinically important as they exceeded the mean clinically important difference (MCID) for each outcome measure. These benefits were maintained at 20 weeks (12 weeks post end of PR programme). Participants in the PR group were encouraged to continue with their exercise programme after completion of the 8 week programme and were offered free gym membership. However, no information was collected on the intensity or frequency of exercise between weeks 8–20 and so it is difficult to draw any conclusions on the maintenance effect. Although this was a small trial, it was sufficiently powered to detect a mean difference in the primary endpoint (ISWT).
Lee et al (2014) conducted a well-powered RCT (n=85) comparing an 8 week supervised exercise programme with a control group who received no intervention.150 Participants were included if they reported dyspnoea on exertion (Modified Medical Research Council Dyspnoea (mMRC) score of ≥1). A mMRC score of 1 equates to getting short of breath when hurrying on level ground or walking up a slight hill. Primary outcomes were exercise capacity (ISWT and 6 min walking distance (6MWD)) and health related quality of life Chronic Respiratory Disease Questionnaire (CRDQ). Secondary outcomes were cough-related quality of life (LCQ) and psychological symptoms (Hospital Anxiety and Depression Scale (HADS)). There was a significant improvement in exercise capacity in the intervention group compared with the control group but these improvements were not sustained at 6 or 12 months. There were also significant improvements in the dyspnoea and fatigue domains of the CRDQ but not the domains of emotional function or mastery. Exercise training did not have an effect on cough-related quality of life or anxiety and depression. There was a statistically significant reduction in the frequency of acute exacerbations in the exercise group (median 1 (IQR1-3)) compared with the control group (2 (1–3)) over 12 months (P=0.012). There was also a statistically significant longer time to first exacerbation in the exercise group of 8 months (95% CI 7 to 9 months) compared with the control group (6 months (95% CI 5 to 7 months) P=0.047). However, these results should be interpreted with caution as a significant number of participants (30/85) that did not complete the 12 month follow-up.
The most recent randomised controlled trial by Olveira et al (2015) (n=30) aimed to assess the effect of a 12 week PR programme versus a PR programme plus a hyperproteic oral nutritional supplement.216 Exercise capacity was not a reported outcome measure. Muscle strength measured using mean handgrip dynamometry was significantly improved in both groups at 12 and 24 weeks. Health-related quality of life assessed using the Quality of Life – Bronchiectasis questionnaire QOL-B Physical Functioning scale significantly improved in the PR plus nutritional supplement group but not in the PR alone group. However, these results should be interpreted with caution for two main reasons. First, there was a large difference in the baseline QOL-B score of the two groups. Although this was not a statistically significant difference, the mean QOL-B score of the PR alone group was more than 12 points lower than the PR plus nutritional supplement group at baseline. In addition, between group statistical analysis was not performed.
An uncontrolled, retrospective study by Van Zeller et al217 (2012) assessed the effect of a 12 week PR programme on 41 participants with bronchiectasis.217 The exercise component consisted primarily of cycle ergometer exercise with additional upper limb and quadriceps training. This does not reflect current UK clinical practice where PR programmes usually include a walking component in order to improve walking function. There was no significant change in 6MWD at the end of the programme. These results are in direct contrast to the aforementioned RCTs which all showed that exercise had a clinically significant effect on exercise capacity.150 214 215
A larger (n=135) and more recent retrospective study evaluated the effect of a 3 week inpatient PR programme on individuals with bronchiectasis.218 This PR programme had a statistically significant effect on 6MWD which improved by 35±43 m (P<0.0001). Health-related quality of life was measured using the EuroQol visual analogue scale (EQ-VAS) and improved by 15±12 (P<0.0001). Dyspnoea was measured with the Baseline/Transition Dyspnoea Index (BDI/TDI) and this also improved after the programme from 7.3±2.9 to 4±2.6 (no p value given). Regression analyses revealed that male gender, baseline FEV1/VC<70% and>2 exacerbations in the previous year were independent predictors of improvement in exercise capacity and health-related quality of life. Although this is a retrospective and uncontrolled study, it does reveal that patients with more severe bronchiectatic disease also benefit from inclusion in a PR programme.
There is currently no evidence assessing the incidence of cross infection of respiratory pathogens between individuals with bronchiectasis in the group exercise setting.
In summary, there is strong evidence from a number of trials to show that PR increases exercise capacity and can improve health-related quality of life in bronchiectasis. One RCT has also shown that PR reduces the frequency of acute exacerbations over a 12 month period and increases the time to first exacerbation, although there are significant methodological issues regarding dropouts.150
Inspiratory muscle training
Two studies investigate the effects of inspiratory muscle training (IMT).214 219 The study by Liaw et al219 found that an 8 week home-based IMT training programme resulted in a significant difference in inspiratory and expiratory muscle strength in the intervention group when compared with the control. However, there were no significant between group differences in any other measure including pulmonary function, quality of life or walking capacity. This study was at high risk of bias due to significant differences between groups at baseline in some measures of pulmonary function and also age. There were a relatively high number of drop outs and intention to treat analysis was not employed. There were 19 participants in each group but six participants dropped out in each group and therefore only 13 participants in each group were included for final analysis. A final consideration is that the participants were not blinded as the control group did not receive any form of sham IMT.
The study by Newall et al214 was well-conducted but had a small number of participants (n=32).214 This study had three groups: PR plus IMT, PR plus sham IMT and a control group which received no intervention. Exercise capacity increased significantly in both the PR-SHAM and PR-IMT groups. HRQOL was significantly better in the PR-IMT group than the PR-SHAM. After 3 months, exercise capacity had declined significantly in the PR-SHAM group but had been maintained in the PR-IMT group. The findings of this study suggest that there is no additional advantage of simultaneous IMT with PR to increase exercise capacity. However, IMT may be important in prolonging the benefit of the training effects.
Field walking tests
Research has now been conducted to support the use of the 6MWT and ISWT as reliable and responsive measures of exercise capacity in the bronchiectasis population (Lee et al).220 This study also found that there was a small learning effect in both measures at baseline and it is therefore recommended that two of each test are performed to accurately assess exercise capacity. In addition, a minimal important difference has been estimated for the 6MWT (25 m) and ISWT (35 m) in bronchiectasis (Lee et al).221 Therefore, these are suitable outcome measures to assess exercise capacity before and after PR in the bronchiectasis population.
Evidence statements
Pulmonary rehabilitation increases exercise capacity and can improve quality of life in individuals with bronchiectasis. (1+)
Pulmonary rehabilitation can reduce frequency of exacerbations over a 12 month period and can increase the time to first exacerbation. (1-)
IMT, when used in conjunction with pulmonary rehabilitation, can enhance the longevity of the training effects. (1+)
IMT in isolation does not increase exercise capacity or quality of life in individuals with bronchiectasis. (1-)
6MWT and ISWT are reliable and responsive outcome measures for use in bronchiectasis to evaluate exercise capacity pre and post pulmonary rehabilitation. (3)
There is currently no evidence assessing the incidence of cross infection of respiratory pathogens between individuals with bronchiectasis in the group exercise setting.
Recommendations
Offer pulmonary rehabilitation to individuals who are functionally limited by shortness of breath (Modified Medical Research Council (MMRC) Dyspnoea Scale≥1). (B)
Consider the use of inspiratory muscle training in conjunction with conventional pulmonary rehabilitation to enhance the maintenance of the training effect. (B)
Good practice points
Educate all individuals with bronchiectasis on the importance of an exercise training programme.
Consider the 6MWT and/or the ISWT when evaluating exercise capacity pre/post pulmonary rehabilitation in bronchiectasis. Prior to this, practice tests should be carried out to eliminate any learning effect.
Pulmonary rehabilitation providers should offer education sessions tailored to the needs of individuals with bronchiectasis (eg, airway clearance techniques, the pathophysiology of bronchiectasis and relevant inhaled therapy).
Pulmonary rehabilitation exercise and education sessions should be provided by appropriately qualified healthcare practitioners.
Further information on Pulmonary rehabilitation is provided in the BTS Quality Standards for Pulmonary rehabilitation (https://www.brit-thoracic.org.uk/standards-of-care/quality-standards/bts-pulmonary-rehabilitation-quality-standards/)
Research recommendation
The role of education, self management plans and who delivers the pulmonary rehabilitation needs to be explored.
The role of pulmonary rehabilitation after exacerbations requiring hospital admission needs to be explored.
The incidence of cross-infection of respiratory pathogens in the group exercise setting should be investigated in the bronchiectasis population.
What is the role of surgery in managing bronchiectasis?
Multiple case series of surgical resection for bronchiectasis are available.222–237 A Cochrane review concluded there are no high quality randomised control studies and the benefits of surgery over conservative management were unclear. It is also likely there is a reporting bias for the available case series.238
Generally surgery should not be considered until there is optimisation of medical management. With this caveat the consistency of available evidence supports a role for surgery in bronchiectasis in selected patients.
The indications for surgical resection in bronchiectasis include
persistent symptoms despite up to a year of comprehensive medical treatment,
exacerbations that are either severe or frequent and interfere with social/professional life,
recurrent refractory or massive haemoptysis,
post obstruction bronchiectasis distal to tumours
localised severely damaged lobe/segment that may be a source of sepsis that left in situ may lead to extension of lung damage.
Surgery is generally applied when there is focal disease in the presence of the above clinical scenarios. Therefore the population both requiring and suitable for surgery is likely to be small. Notably many series reported to date included patients with a lower mean age than seen in many clinics, ranging from 30 to 48 years of age.222 225 239 The median duration of symptoms prior to surgery in the reported series was usually prolonged e.g. 6 years.225
A variety of operative techniques have been described. In experienced hands video assisted thoracoscopic (VAT) performs as well as open surgery231 233 239 and may be associated with lower rates of complications such as blood loss and shorter hospitalisations.233 There is however an intraoperative conversion rate from VATS to open surgery of up to 12%.233 The resection limits range from segmentectomy to pneumonectomy but the available literature does not provide robust decision making tools to aid decision making on the optimal resection limits in day to day practice.222 225 231 233 239
With this in mind pre-surgical safety assessment should be undertaken to define the expected amount of residual lung, underlying cardiopulmonary reserve and anticipated overall risks. Pulmonary rehabilitation and optimisation of nutrition are important aspects with which respiratory physicians can support their patients.
In the available series the 60 day mortality outcomes ranged from 0%–11%.224 232 237 239 Common post-operative complications included wound infection, empyema, systemic sepsis, post thoracotomy pain, prolonged air leak and recurrence of bronchiectasis.224–226 234 235 Early morbidity rates ranged from 13% to 24%222 225 232 235 239 with wound infection reported as the most common complication (6%) in one large series of 277 patients.240
For long term complications the recurrence rate is likely to depend on the completeness of resection and underlying aetiology of bronchiectasis. Perceived complete resection is associated with significantly better long term outcomes than cases where incomplete resection has occurred.223 225 232 239 240 In one small case series of 31 patients, the mean time to recurrence of symptoms was 34 months.232 An immunocompromised status, persistent infection with P. aeruginosa and the extent of residual bronchiectasis after surgery have been associated with a significantly shorter recurrence-free interval.232 The primary cause of bronchiectasis may influence post-surgical outcomes with likely better outcomes after post obstructive bronchiectasis and poorer outcomes in immunodeficiency.232 There are however limited data to guide clinicians in defining risk benefit ratios.229 238 Even when the primary cause of bronchiectasis persists, successful outcomes are reported. Surgery can be successful in primary ciliary dyskinesia.226
Freedom from symptoms of bronchiectasis have reported as high as 61%–84% when followed up from between 1 to 5 years or more post-operatively.224 225 234
Evidence statement
Surgery may be successful in bronchiectasis in reducing exacerbations or treating haemoptysis. (3)
The ideal candidate(s), timing for surgery and operative approach remain ill-defined. (3)
Video assisted thoracoscopic technique can provide outcomes at least as successful as open surgery. (3)
Improvements in bronchiectasis symptoms can be seen after surgery for bilateral disease. (3)
Recommendations
Consider lung resection in patients with localised disease whose symptoms are not controlled by medical treatment optimised by a bronchiectasis specialist. (D)
Offer multidisciplinary assessment, including a bronchiectasis physician, a thoracic surgeon and an experienced anaesthetist, of suitability for surgery and pre-operative assessment of cardiopulmonary reserve post resection. (D)
Good practice point
Consider nutritional support and pre-operative pulmonary rehabilitation before surgical referral.
Lung transplantation for bronchiectasis
Lung transplantation is an effective therapy for bronchiectasis when maximal medical therapy is failing. Lung transplantation is generally reserved for those with diffuse bilateral disease and bilateral transplantation is then performed. There are however reports of single lung transplantation with contralateral pneumonectomy. Generally lung transplantation is felt indicated where survival is anticipated at 50% at 2 years without lung transplantation.241 International guidelines note the risks of transplantation in general appear to increase with age and generally patients above the age of 65 are felt to have an unfavourable risk: benefit mortality ratio.241
Internationally bronchiectasis is reported as a rare indication for lung transplantation representing less than 5% of all bilateral lung transplantations recorded in the international registry. Overall less than 1200 transplant procedures for bronchiectasis were recorded in the international registry as compared with 1280 for pulmonary hypertension, 6862 for cystic fibrosis and 13 672 for COPD (https://www.ishlt.org/registries/slides.asp?slides=heartLungRegistry accessed Aug 2015).
The available case series focus on lung transplantation for adults with bronchiectasis with no significant data reported for paediatric transplantation. While collectively less than 200 patients, these case series report good outcomes following transplantation. In a case series of 22 patients transplanted in the UK between 1988 and 2001 undergoing bilateral lung transplantation either as bilateral sequential single-lung transplants (BSSLTX), heart-lung transplants (HLTX) or single-lung transplants (SLTX) the reported outcomes included lung function and mortality data.242 Overall the 1 year Kaplan-Meier survival for all patients was 68% (95% CI, 54% to 91%), with the 5 year survival reaching 62% (95% CI, 41% to 83%). In those undergoing SLTX for bronchiectasis the 1 year survival was lower at 57% (95% CI, 20% to 94%) compared with those receiving 2 lungs 73% (95% CI, 51% to 96%). At 6 months, mean forced expiratory volume in 1 s was 73% predicted (range, 58%–97%), and mean forced vital capacity was 68% predicted (range, 53%–94%) after receiving two lungs (n=10).
A small single centre case series of 37 patients from Cambridge, UK reported transplantation outcomes in those with bronchiectasis due to immunodeficiency syndromes (n=5, predominantly antibody deficiency patients on replacement therapy) compared with other causes of bronchiectasis (n=32).243 The actuarial survival was comparable between the two groups. The 1 year survival was 81% in the bronchiectasis group and 80% in bronchiectasis-antibody deficiency recipients. Functional outcomes following transplant were good with the FEV1 (mean +/-SD) at 1 year post transplant being 83.7%+/-24.2% in the bronchiectasis group and 83.0%+/-30.4% in the bronchiectasis-antibody deficiency recipients.
A single centre experience of 17 bronchiectasis patients from Madrid, Spain reported that in a series of 171 patients, 44 (26%) were transplanted for suppurative lung diseases.244 Of these 27 had cystic fibrosis (61%) and 17 (39%) were classified as bronchiectasis. The reported survival of cystic fibrosis patients was 85% at 1 year and 45% at 5 years while that of bronchiectasis patients demonstrated an initially higher mortality rate (survival 70% at 1 year) but similar long term survival (54% at 5 years). P. aeruginosa infection in pre-transplant recipients was common but not invariable. No clear association was seen between pre transplant P. aeruginosa and poorer post transplant outcomes, though the study was unlikely to be powered. Persistence of the pre-transplant infecting organism was common at 1 year following transplantation.244
One study of over 1000 patients in the UK waiting for lung transplantation included adults with cystic fibrosis (n=430), bronchiectasis (n=123), pulmonary hypertension (n=74), diffuse parenchymal lung disease (n=564), chronic obstructive pulmonary disease (COPD n=647) and miscellaneous indications (n=159). The proportion of patients in each group who died while on an active transplant list listed varied significantly (respectively 37%, 48%, 41%, 49%, 19%, 38%). Hence these data demonstrate that bronchiectasis has one of the highest ‘on-list’ mortality rates with up to 60% mortality on list at 2 years.245
Furthermore in the 54 of 123 bronchiectasis patients on the waiting list that survived to transplantation, median survival was 3001 days which was better post-transplant survival rates than more common indications for transplantation such as COPD (n=483 transplanted, median survival 1795 days) and cystic fibrosis (n=234, 2436 days).245
Consistent with international guidelines, those transplanted had severe disease (mean FEV1 26% predicted) and were younger than the median age of patients reported in the UK national audit of outpatient bronchiectasis with average age at transplantation 49.7 years.245
Evidence statement
As stated in international Lung transplantation guidelines, post-transplant morbidity and mortality increase with age and hence transplantation is in general reserved for those aged 65 years or less. (3)
In selected patients with bronchiectasis, lung transplantation improves quality of life and is associated with post-transplant survival of over 60% at 5 years. (3)
Bronchiectasis patients have poor outcomes on lung transplant waiting lists with mortality rates of up to 60% at 2 years. (3)
The majority of transplantation procedures performed for bronchiectasis are bilateral lung transplants in patients with severely impaired quality of life or rapid deterioration. (3)
Recommendation
Consider transplant referral in bronchiectasis patients aged 65 years or less if the FEV1 is <30% with significant clinical instability or if there is a rapid progressive respiratory deterioration despite optimal medical management. (D)
Consider earlier transplant referral in bronchiectasis patients with poor lung function and the following additional factors: massive haemoptysis, severe secondary pulmonary hypertension, ICU admissions or respiratory failure (particularly if requiring NIV). (D)
Good practice points
Discuss appropriate patients with a transplant centre prior to formal referral.
Optimise management of comorbidities such as osteoporosis and maintaining physical condition through pulmonary rehabilitation prior to transplant.
What is the role of influenza and pneumococcal vaccination in management of bronchiectasis
Influenza vaccination
There are no randomised controlled trials evaluating the impact of annual influenza vaccination on respiratory exacerbations and pulmonary decline in adults with bronchiectasis.246 Evidence for the potential benefits of influenza vaccination may be derived from studies of patients with chronic obstructive pulmonary disease (COPD), some of whom will also have bronchiectasis. In a systematic review of influenza immunisation in COPD, administration of inactivated influenza vaccines in placebo-controlled randomised controlled trials was associated with reduced late exacerbations (Weighted Mean Difference −0.39, 95% CI −0.61 to −018) and laboratory confirmed influenza infection (Odds Ratio-0.19, 95% CI −0.07 to −048) in COPD patients.247 Observed reduction in exacerbations of COPD was due to fewer influenza infections occurring 3 weeks or more after influenza immunisation. Vaccination did not cause an increase in short term exacerbation (within 2 weeks of immunisation) but was associated with a transient increase in injection site pain and redness. Influenza vaccination had no impact on hospitalisation, mortality, lung function and exercise tolerance however the number of studies assessing some parameters (hospital admissions, death rates) was very small and hence type two statistical error cannot be excluded. Although there are few randomised controlled trials of influenza vaccination in COPD, the results of such studies are consistent with those observed in large retrospective cohort studies.247
Pneumococcal vaccination
There is limited evidence supporting the use of 23 valent pneumococcal vaccine to prevent exacerbations of bronchiectasis.248 One randomised controlled trial comparing pneumococcal and influenza vaccination versus influenza vaccination alone in patients with chronic lung disease including COPD and bronchiectasis showed that patients given the 23 valent pneumococcal vaccine had fewer exacerbations.249 The NNV was 6 (95% CI 4 to 32) over 2 years. No difference between groups was observed for pneumonia incidence, and pulmonary function test data were not reported. The limitations of this study include open label design, small number of patients with bronchiectasis enrolled (n=20), lack of microbiological evidence for pneumococcal infection and failure to document severity of chronic lung disease.
Randomised controlled trials show that 23 valent pneumococcal vaccination can prevent all cause pneumonia (OR 0.72 95% CI 0.56 to 0.93).250 There is however marked statistical heterogeneity between studies, according to study site (high income v low income countries), population (healthy adults v those with chronic medical illnesses) and the pneumococcal vaccine used (14 valent v 23 valent). The 23 valent pneumococcal vaccine was effective against all cause pneumonia in low income countries (OR 0.54 (5% CI 0.43 to 0.67) but in high income countries, studies in healthy adults and in those with chronic medical illnesses were negative.250 The 23 valent pneumococcal vaccine is still offered in the UK, based on the evidence that, for adults between the ages of 65–74 with chronic lung disease, the 23 valent polysaccharide pneumococcal vaccine continues to provide short term protection against invasive pneumococcal disease and remains cost effective.251 252
The role of protein conjugate pneumococcal vaccination is contentious. There is no evidence as to the efficacy of protein conjugate pneumococcal vaccination in patients with bronchiectasis.
Evidence statements
The potential benefit of influenza vaccination in reducing exacerbations and influenza infection is derived from studies of individuals with COPD, some of whom will also have bronchiectasis. In the absence of direct evidence, influenza vaccination can be justified based on individual patient needs (presence of COPD, immune deficiency, nursing home residence, patient preference and expert opinion) and adherence to national guidelines. (4)
The 23 valent polysaccharide pneumococcal vaccination with influenza immunisation may reduce exacerbations of bronchiectasis. (1-)
Meta-analysis of RCTs supported the use of 23 valent pneumococcal vaccine in reducing the rate of all cause pneumonia in healthy adults and those with chronic illnesses although there was marked statistical heterogeneity. (1+)
Recommendations
Offer annual influenza immunisation to all patients with bronchiectasis. (D)
Offer polysaccharide pneumococcal vaccination to all patients with bronchiectasis. (D)
Good practice point
Consider influenza vaccination in household contacts of patients with immune deficiency and bronchiectasis to reduce the risks of secondary transmission.
Consider use of 13 valent protein conjugate pneumococcal vaccine in patients with bronchiectasis who do not have an appropriate serological response to standard polysaccharide vaccine (23 valent carbohydrate Pneumococcal vaccine).
Treatment of respiratory failure
A study of survival of 48 patients in the intensive care unit (ICU) where one of the interventions was NIV (n=13, 27%) found cumulative mortality of 19% (n=9) for a first admission to ICU for respiratory failure in patients with bilateral non-CF bronchiectasis and 40% (n=19) at 1 year.253 The actuarial survival rate at 1 year was 60%. Intubation requirement was associated with reduced survival in univariate analysis, suggesting that NIV may be advantageous. Multivariate analysis found that age >65 years and long-term oxygen therapy were independent factors predicting reduced survival. Survival was not increased for those treated with long-term non-invasive positive pressure ventilation. A retrospective analysis of patients treated with non-invasive (n=31) versus invasive (n=26) ventilation for respiratory failure reported a 32% failure rate with NIV for progression to IV or death.254 The overall in hospital mortality was around 25%, not different between NIV and IV, and predicted by APACHE score. Bronchiectasis in the context of COPD may increase the duration of ICU stay (median 14 vs 9 days) but did not influence mortality in a study of 93 patients with COPD on invasive ventilation, 31% of whom had radiological bronchiectasis.255
A study of the outcome of domiciliary NIV noted that the response to NIV in this group of patients (n=13) was disappointing.256 The patient group had more severe hypoxaemia and hypercapnia at the start, suggesting that NIV was introduced later in the natural history of the disease than in previous studies. The probability of continuing NIV after 2 years in the bronchiectasis group was <20% and most patients became increasingly more ventilator dependent with time. However, all reported improvement in quality of sleep and in levels of daytime activity. Eight considered that the improvement in their respiratory status outweighed the discomfort due to NIV.
A retrospective study of 16 patients with severe diffuse bronchiectasis investigating NIV as rescue therapy for nocturnal home use with daytime oxygen found a significant increase in FEV1 12 months after initiation of NIV. In patients alive after 24 months there was a significant decrease in the length of hospital admissions.257 This could be a reflection of the three deaths being the high intensity users.
In a study which compared patients with bronchiectasis treated with NIV with those treated with long-term oxygen therapy only, differences were found between the two groups. In the year before NIV was commenced, mean/SD length of time in hospital for the NIV and long-term oxygen therapy groups was 48+/-55 and 5+/-8 days, respectively; the year following home NIV the length of time in hospital for the two groups was 10+/-31 and 9+/-16 days, respectively.258 In contrast, a further study did not find a reduction in hospital days with the instigation of non-invasive positive pressure ventilation in patients with bronchiectasis.259
Evidence statements
There are no specific studies of LTOT for respiratory failure in bronchiectasis, but expert opinion based on data in COPD is that this is likely to be a beneficial intervention. (4)
NIV may lead to a reduction in hospitalisation days in patients with bronchiectasis and hypercapnic respiratory failure however the proportion of patients remaining on NIV at 2 years is low. (3)
Recommendations
Consider long term oxygen therapy for patients with bronchiectasis and respiratory failure, using the same eligibility criteria as for COPD. (D)
Consider domiciliary non-invasive ventilation with humidification for patients with bronchiectasis and respiratory failure associated with hypercapnia, especially where this is associated with symptoms or recurrent hospitalisation. (D)
Bronchiectasis and other treatments: cough suppression, nutritional supplements, complementary therapy/homeopathy, supplemental treatments
The majority of studies of alternative therapies and bronchiectasis are mainly observational with small patient numbers. There is a lack of randomised controlled trials.
A small (n=35) randomised, partially blinded study (over 8 weeks) involving three groups, on the role of self-administered acupressure to reduce the symptoms of bronchiectasis and improve QOL.260 The three groups were standard care +self administered acupressure (n=11), standard care +sham acupressure (n=11) (not applied to real acu-points) and standard care alone (n=13). All aged 40–70 years (sex not identified). Originally 49 enrolled, 12 dropped out by week 4, 2 by week 8.
The findings showed that after 8 weeks of self-administered acupressure seemed to be useful in reducing the effects of bronchiectasis on patients’ daily activities, however, the authors conceded that sham acupressure administered for the same amount of time was capable of improving some of the symptoms of bronchiectasis. A Cochrane review, Singing for children and adults with bronchiectasis, found no eligible trials, therefore, no data were available for analysis.261 A review262 and a controlled study263 around vitamin D both concluded that vitamin D deficiency was common in bronchiectasis, however, there were no RCTs assessing vitamin D. A case control study on a small number of patients (n=34 with bronchiectasis, n=29 without) found that the patients with bronchiectasis had significantly lower serum zinc level than the control group, however, there were no trials to evaluate the prophylactic or therapeutic use of zinc supplements.264
Evidence statement
Alternative treatments such as complementary therapy/homeopathy and supplemental treatments have limited evidence to support their use.
Recommendation
Do not routinely recommend alternative treatments (for example cough suppression, nutritional supplementation, complementary therapy/homeopathy, supplemental treatments) as part of the management of patients with bronchiectasis. (D)
Good practice point
Record patient’s weight and BMI at each clinic appointment.
Research recommendations
Further interventional/randomised controlled trials needed to establish the role of any alternative therapies in the management of bronchiectasis.
Studies assessing the benefits of nutritional supplementation in patients with bronchiectasis should be undertaken.
Section 10
Do pathogens have an impact on prognosis in bronchiectasis?
In UK studies, the most frequent pathogen isolated from traditional culture in bronchiectasis is Haemophilus influenzae (20%–40%), followed typically by P. aeruginosa (10%–30%), Moraxella catarrhalis, Streptococcus pneumoniae, Staphylococcus aureus and enterobacteriaceae.68 120 265 266 Patients with NTM account for 1%–10% of cases.267 268
There is a clear and consistent association between the presence of P. aeruginosa and poor outcome. All studies that have examined this outcome conclude that P. aeruginosa is associated with a three-fold or greater increased risk of mortality, even after adjustment for potential confounders.120 266 269 270
Patients with P. aeruginosa are also more likely to require hospital admission due to a greater disease severity and a more frequent requirement for intravenous antibiotic treatment, either due to outpatient antibiotic failure or antibiotic resistance.120 Patients with P. aeruginosa colonisation also have worse health related quality of life using the St. Georges Respiratory Questionnaire, more frequent exacerbations, and worse lung function in cross-sectional studies.120 265 271–273
The relationship between P. aeruginosa and lung function decline has been evaluated in relatively few patients and shows inconsistent results. Two studies show no relationship between P. aeruginosa and FEV1 decline,15 274 while two show a significant relationship.271 275 Therefore no firm conclusion on this relationship can be made without further studies.
There is less evidence for a prognostic impact of organisms other than P. aeruginosa. One large study shows that colonisation with any organism other than P. aeruginosa is associated with a poorer outcome compared with patients not colonised with pathogens.120
There is limited data on prognosis with specific pathogens such as NTM and A. fumigatus.267 268 276 There is a consistent relationship between airway bacterial load and airway inflammation across several studies using both sputum and bronchial wash.168 277 278
An increasing number of studies using molecular techniques to characterise the airway microbiome are being published.279 280 Microbiome studies demonstrate that loss of bacterial diversity is associated with worse disease defined by FEV1 or exacerbation frequency.279 While this has been a valuable research tool, at present this is not available for daily practice and the extent to which it provides clinically relevant information beyond that available from culture has not been established.
Evidence statements
Chronic colonisation with P. aeruginosa is independently associated with
Higher mortality during follow-up (2++)
Higher risk of admissions to hospital (2++)
Increased exacerbations (2++)
Poorer quality of life (2++)
Worse radiological severity of disease (2+)
Lower FEV1 and FVC cross-sectionally (2++)
Chronic colonisation with pathogens other than P. aeruginosa are associated with
Hospital admissions (2++)
Greater airway inflammation (2++)
Sputum bacterial load is associated with
Greater airway inflammation (2++)
More frequent exacerbations and hospital admissions (2+)
Recommendations
Consider patients with chronic P. aeruginosa colonisation at higher risk of bronchiectasis-related complications. (B)
Perform regular sputum microbiology screening for patients with clinically significant bronchiectasis to monitor for pathogens and detect new isolation of P. aeruginosa. (C)
Section 11
What is the evidence for the role of viruses/fungal disease in patients with bronchiectasis?
A single prospective study has reported on the prevalence of respiratory viruses in adult patients with bronchiectasis. Nasopharyngeal swabs and sputum samples, collected from 119 patients at baseline, when clinically stable and at exacerbation, were assayed for 16 respiratory viruses. Viruses were found more frequently in nasopharyngeal swabs and sputum during exacerbations (49/100, 49.0%) than during steady state (11/58, 19%). Virus-positive exacerbations were associated with a greater increase in markers of systemic and airway inflammation but no differences in lung function, quality of life, and bacterial density were apparent.281
Similarly, data regarding the potential role of fungi in bronchiectasis is lacking. A retrospective cohort study was performed using 252 patients from 4 Centres in Spain.282 All patients had at least one sputum sample cultured for fungi, with a mean ±SD of 7±6 cultures per patient. Persistent Aspergillus spp. and C. albicans were defined as the presence of 2 or more positive sputum cultures for Aspergillus spp. and C. albicans, respectively, taken at least 6 months apart; eighteen (8.7%) and 71 (34.5%) patients had persistent positive cultures for Aspergillus spp. and C. albicans, respectively. Logistic regression, to determine the most significant predictors of fungal persistence, revealed that the presence of mucopurulent or purulent sputum was associated with persistence of Aspergillus spp. with long-term antibiotic therapy associated with persistence of C. albicans.
Evidence statement
There is insufficient evidence to evaluate the role of fungi and viruses in patients with bronchiectasis. (2-)
Good practice points
Testing to detect viral infection should be considered in patients with an exacerbation of bronchiectasis.
Do not routinely use anti-fungal therapy without evidence of fungal disease. Fungal cultures can be positive on those receiving long-term antibiotic therapy.
Section 12
Does eradication of potentially pathogenic microorganisms improve outcomes in patients with stable bronchiectasis?
There is one randomised controlled study that directly addresses whether antibiotic treatment following first isolation of P. aeruginosa improves outcomes in patients with bronchiectasis. Six RCTs report the frequency of negative cultures following antibiotic treatment and one retrospective study reports the outcomes of antibiotic regimens prescribed specifically for P. aeruginosa eradication.
In a randomised, but unregistered, study evaluating the effect of 2 weeks of ceftazidime and tobramycin followed by either nebulised tobramycin 300 mg (Tobi) or placebo twice daily for 3 months in 35 patients with bronchiectasis and a first growth of P. aeruginosa, the median time to recurrence of P. aeruginosa was higher (P=0.048) in the nebulised tobramycin group (n=11) compared with placebo group (n=17), with the proportion free of P. aeruginosa after 12 months follow-up being 55% and 29%, respectively.283 The number of exacerbations (1.27±1.62 vs 2.5±1.63, P=0.04), the number of hospital admissions (0.06±0.25 vs 0.47±0.51, P=0.04) and the number of days in hospital (0.90±3.01 vs 13.56±22.64, P=0.03) were also significantly lower in the nebulised tobramycin group. Five patients in the nebulised tobramycin group discontinued treatment due to bronchospasm and two patients in the placebo group withdrew from the study.
In a randomised single blind trial evaluating the effect of nebulised gentamicin in patients with bronchiectasis, negative sputum cultures after 12 months treatment were more common in the gentamicin group (18/27, 67%) compared with the control group (1/30, 3%).201 However, a lesser treatment effect was seen in patients with P. aeruginosa at baseline, with 7/13 (54%) gentamicin treated patients and 9/12 (75%) control patients reculturing the organism after 12 months treatment. In the whole group, gentamicin treatment was also associated with less sputum purulence (9% vs 39%; P<0.0001); greater exercise capacity (510 (350–690) m vs. 415 (268–530) m; P=0.03); and fewer exacerbations (0 (0–1) vs. 1.5 (1-2); P<0.0001) with increased time to first exacerbation (120 [87–162] days vs. 62 [21–123] days; P=0.02). The gentamicin group had greater improvements in Leicester Cough Questionnaire (81% vs 20%; P<0.01) and St. George's Respiratory Questionnaire (88% vs 19%; P<0.004) score. However, 3 months after treatment cessation, all outcome measures were similar to baseline.
In a randomised double blind placebo controlled trial evaluating the effect of dual release liposomal ciprofloxacin in patients with bronchiectasis and ciprofloxacin sensitive P. aeruginosa, failure to culture P. aeruginosa after 28 days treatment was more common in the ciprofloxacin group compared with the control group (12 (60%) vs 3 (14%), OR 9.5, 95% CI 1.8 to 63.0, P=0.003).199 In the per protocol analysis, time to first exacerbation was delayed in the ciprofloxacin group compared with the placebo group (134 vs 58 days, P=0.046).
In a randomised double blind placebo controlled trial evaluating the effect of dry powder ciprofloxacin in patients with bronchiectasis and predefined potential respiratory pathogens including P. aeruginosa and H. influenzae, negative bacterial cultures after 28 days treatment was more common in the ciprofloxacin group compared with the placebo group (14 (35%) vs 4 (8%), P=0.001).198
In a 12 month randomised double blind placebo controlled trial evaluating the effect of erythromycin in patients with bronchiectasis, eradication of pathogens (defined as a negative end of treatment sputum culture in participants with pathogenic bacteria identified in baseline samples) occurred more commonly in the erythromycin group compared with the placebo group (17 (30%) vs 6 (11%), OR 3.6, 95% CI 1.3 to 10.6, P=0.01).192 Overall, erythromycin treated patients also had fewer protocol defined pulmonary exacerbations, a lower 24 hours sputum volume and a smaller lung function decline over 12 months compared with controls. However, two contemporary RCTs evaluating the effect of azithromycin in patients with bronchiectasis found no difference between azithromycin and placebo treated patients regarding the eradication of respiratory pathogens (despite there being significant clinical benefits associated with azithromycin treatment)190 191 and two subsequent meta-analyses of macrolide trials in this patient population found no overall benefit in this respect.193 196
A retrospective study assessed the clinical and microbiological outcomes of eradication therapy following initial P. aeruginosa isolation.284 Eradication therapy involved intravenous antibiotics (n=12), intravenous antibiotics followed by oral ciprofloxacin (n=13), or ciprofloxacin alone (n=5), combined with 3 months of nebulised colistin. P. aeruginosa was eradicated from sputum in 24 patients (80.0%). While 11/24 (46%) subsequently recultured P. aeruginosa (median time 6.2 months), isolates were not genotyped to assess whether this represented relapse or reinfection. Exacerbation frequency was significantly reduced from 3.9 per year pre-eradication to 2.1 post-eradication (P=0.002). Admission rates were unchanged. 20/30 patients reported initial clinical improvement, while at 1 year follow-up, 19/21 had further improved or remained stable. Lung function was unchanged.
Patients with bronchiectasis may also culture a number of other drug resistant pathogens such as MRSA, Stenotrophomonas maltophilia and Achromobacter species.280 While it is not known if antibiotics prescribed following first isolation reliably result in eradication or improved patient outcomes, in clinical practice antibiotics are often prescribed in an attempt to prevent chronic infection.
A recent meta-analysis of eight randomised controlled trials recruiting 539 patients showed that long-term inhaled antibiotics reduced sputum bacterial density and augmented eradication of sputum P. aeruginosa. No evidence showed higher risk of P. aeruginosa resistance after inhaled therapy. In addition, nebulized therapy reduced the number of patients with exacerbation. However, patients with inhaled antibiotics were more likely to suffer wheeze and bronchospasm.207
In summary, the available RCT data suggest that inhaled antibiotics improve outcomes in patients with bronchiectasis and that a proportion of patients’ cultures convert as a result of treatment. However, only one RCT evaluated outcomes of treatment prescribed to eradicate the first growth of a microorganism. The most clinically relevant definition of eradication has not been established (single negative culture vs sequential negative cultures vs negative PCRs); and it is not known if true bacterial eradication is an achievable endpoint in patients with bronchiectasis, nor whether it is superior to reducing bacterial density at improving patient outcomes. Apparent clearance of P. aeruginosa is achieved in some studies. However, the most cost effective antibiotic regimen has not been established, nor whether relapse occurs due to re-emergence of the original strain or de novo infection. Furthermore, it appears that spontaneous P. aeruginosa clearance can occur, as some patients only culture P. aeruginosa intermittently.266 274
Evidence statements
In patients with bronchiectasis and a first growth of P. aeruginosa, treatment with 2 weeks of intravenous ceftazidime +tobramycin followed by 3 months of nebulised tobramycin (Tobi) results in a higher median time to recurrence of P. aeruginosa, a reduced exacerbation frequency and a reduced admission rate/days in hospital compared with treatment with 2 weeks of intravenous antibiotics followed by 3 months of nebulised 0.9% saline. (1-)
Recommendations
Offer patients with bronchiectasis associated with clinical deterioration and a new growth of P. aeruginosa (1st isolation or regrowth in the context of intermittently positive cultures) eradication antibiotic treatment: (first line treatment: ciprofloxacin 500–750 mg bd for 2 weeks; second line treatment: iv anti-pseudomonal beta-lactam ±an iv aminoglycoside for 2 weeks, followed by a 3 month course of nebulised colistin, gentamicin or tobramycin). (D)
Discuss with patients the potential risks and benefits of starting eradication antibiotic treatment versus clinical observation following a new growth of P. aeruginosa in the context of stable bronchiectasis. This will include consideration of the likelihood of achieving sustained eradication, the risk of developing chronic infection, and the risk of adverse events with each management approach. (D)
Offer patients with bronchiectasis associated with clinical deterioration and a new growth of methicillin-resistant S. aureus (MRSA) (1st isolation or regrowth in the context of intermittently positive cultures) eradication. This should be attempted especially in view of infection control issues. (D)
Good practice point
Send sputum for culture and sensitivity immediately before and at each clinical attendance following antibiotics prescribed for bacterial eradication to determine the outcome of treatment.
Research recommendation
A randomised control trial of P. aeruginosa eradication therapy is needed to determine the microbiological and clinical outcomes of eradication therapy.
Section 13
Exacerbations
Does antibiotic therapy improve outcomes in patients with an exacerbation of bronchiectasis?
Antibiotics are used to treat exacerbations that present with an acute deterioration (usually over several days) with worsening local symptoms (cough, increased sputum volume or change of viscosity, increased sputum purulence with or without increasing wheeze, breathlessness, haemoptysis) and/or systemic upset.
There are no randomised placebo-controlled studies evaluating the efficacy of antibiotics in exacerbations in adults. An RCT performed by Bilton et al285 compared oral ciprofloxacin (in treatment doses) plus placebo to oral ciprofloxacin plus inhaled tobramycin. The addition of inhaled tobramycin led to improved microbiological outcome but the inability to demonstrate an additional clinical benefit may have been due to emergent wheeze resulting from treatment. A case control study by Chalmers et al demonstrated antibiotics led to a reduction in airway inflammatory markers but no clinical endpoints were reported and there was no follow-up beyond 2 weeks.168
Cohort studies by Murray et al286 and Bedi et al287 showed that in patients that needed intravenous antibiotic therapy according to the BTS guidelines 2010, they had a good clinical response. There was, however, no control group that did not receive antibiotic therapy.
Evidence statement
There is insufficient evidence to evaluate the efficacy of antibiotics in exacerbations in adults with bronchiectasis. (2-)
Good practice points
A patient self management plan should be considered, an example is provided here https://www.brit-thoracic.org.uk/standards-of-care/quality-standards/bts-bronchiectasis-quality-standards/)
There should be prompt treatment of exacerbations and suitable patients should have antibiotics to keep at home.
Previous sputum bacteriology results can be useful in deciding which antibiotic to use. Table 6 highlights the first-line and alternative treatments for the common bacterial pathogens implicated in exacerbations of bronchiectasis.
Where possible, sputum (spontaneous or induced) should be obtained for culture and sensitivity testing prior to commencing antibiotics.
Empirical antibiotics can then be started while awaiting sputum microbiology.
Once a pathogen is isolated, antibiotics can be modified if there is no clinical improvement, with treatment guided by antibiotic sensitivity results.
In general, antibiotic courses for 14 days are standard and should always be used in patients infected with P. aeruginosa. Shorter courses may suffice in patients with mild bronchiectasis.
Intravenous antibiotics should be considered when patients are particularly unwell, have resistant organisms or have failed to respond to oral therapy (this is most likely to apply to patients with P. aeruginosa).
Section 14
Specific treatments
What treatments improve outcomes in patients with bronchiectasis and Allergic Broncho-Pulmonary Aspergillosis (ABPA)?
Limited evidence suggests that if clinical and immunological features of ABPA are identified before radiological features are present, without evidence of proximal bronchiectasis, progressive lung damage occurs rarely once treatment is started.288
There are no studies to identify how many patients with bronchiectasis are sensitised to A. fumigatus or have seropositive ABPA.
The aims of treatment of ABPA are to control symptoms, prevent and treat exacerbations, reduce inflammation and prevent further progression and damage to the lung.289
The mainstay of treatment is immunosuppression with corticosteroids, with or without the addition of antifungal agents.
Oral corticosteroids
There are no randomised controlled trials of corticosteroid use in patients with ABPA and bronchiectasis.
Corticosteroids are the mainstay of therapy. Starting and maintenance doses vary in the literature.
A tapering dose of corticosteroid is usually used with monitoring of total serum IgE every 6–8 weeks as a marker of disease activity. Regimes vary from Prednisolone, 0.5 mg/kg/d, for 1–2 weeks, then on alternate days for 6–8 weeks before tapering by 5–10 mg every 2 weeks and discontinue290 to more prolonged courses of Prednisolone, 0.75 mg/kg, for 6 weeks, 0.5 mg/kg for 6 weeks, then tapered by 5 mg every 6 weeks to continue for a total duration of at least 6 to 12 months.81 291
Patients are considered in remission when they remain without pulmonary infiltrates and/or eosinophilia for 6 months after oral steroid withdrawal.290
Inhaled corticosteroids
Inhaled corticosteroids (ICS) provide a theoretical advantage to oral corticosteroids (OCS) by minimising systemic effects.
The role of high dose ICS was evaluated in a retrospective study of patients with seropositive ABPA and asthma. The conclusion was that there was no role for ICS in isolation as a treatment although they could provide a useful adjunct alongside oral steroids to better control asthma symptoms.292
Other small case studies had suggested a role for ICS in weaning patients from high doses of OCS who were otherwise difficult to wean with reported relapses in disease activity when doses of OCS were reduced.293
There is no data to support or refute the use of ICS in patients with ABPA and bronchiectasis.
Intravenous corticosteroids
There are very few studies evaluating the role of pulsed IV steroid therapy in ABPA and none in bronchiectasis with ABPA.
A study of pulsed therapy with monthly intravenous methylprednisolone, in conjunction with itraconazole, in nine patients with CF and ABPA was shown to be effective with all patients showing clinical and laboratory improvement - FEV1 increase, serum IgE levels and total eosinophil counts.294 There is no evidence to support the use of IV steroid in patients with ABPA and bronchiectasis.
Azoles
Itraconazole has been shown in a randomised controlled trial to reduce the need for corticosteroids with fewer exacerbations requiring oral corticosteroids in those treated with itraconazole than in the placebo group.295
Other studies of patients with asthma and ABPA have suggested a reduction or elimination of glucocorticoid use while on itraconazole.296
A Cochrane review of the role of azoles in ABPA associated with asthma concluded that itraconazole modifies the immunologic activation associated with ABPA and improves clinical outcome, at least over a period of 16 weeks, but noted that adrenal suppression with inhaled corticosteroids and itraconazole is a potential concern.297
In current UK practice, itraconazole is used for patients who are steroid dependent and for those who have relapsed after a course of steroids. On occasion it has been utilised from the outset in conjunction with commencement of steroid therapy. The recommended adult dose for itraconazole is 100–200 mg twice daily.289
A systematic review of the efficacy and safety of antifungal treatments in patients with ABPA and either asthma or cystic fibrosis, including itraconazole, voriconazole, posaconazole, ketoconazole, natamycin, nystatin and amphotericin B, concluded that there was an improvement in symptoms, frequency of exacerbations and lung function in most of the studies and this was seen more commonly with the azoles.298
There is however a lack of controlled studies evaluating the use of antifungal agents.
Voriconazole and posaconazole are reported to be an effective adjunct therapy in the management of ABPA, with clinical improvement in 70% of patients with ABPA treated with voriconazole and 78% of patients with ABPA treated with posaconazole in studies concerning patients with severe asthma.299
There are no studies concerning the use of these antifungals in patients with bronchiectasis.
Amphotericin B and anti-IgE therapies
The potential role of agents such as amphotericin B and monoclonal antibody therapy with agents such as omalizumab, are of interest but require further evaluation in ABPA.
Monitoring response to treatment
Monitoring response to treatment through repeat measurement of Aspergillus serology, eosinophils and repeat chest radiology can aid weaning of treatment. A study of 81 patients with bronchiectasis and ABPA suggested that the reduction in total IgE was most sensitive to change and most reflective of successful treatment.79
Evidence statements
Itraconazole use in corticosteroid dependent patients is associated with a reduction in corticosteroid dose, improved pulmonary function and improved exercise capacity. (1+)
Total IgE is the most sensitive marker for monitoring treatment response. (2+)
Recommendations
Offer oral corticosteroid to patients with active ABPA. An initial dose of 0.5 mg/kg/d for 2 weeks is recommended. Wean steroids according clinical response and serum IgE levels. (D)
Consider itraconazole as a steroid sparing agent for patients dependent on oral corticosteroids where difficulty in weaning is experienced. (B)
Monitor patients with active ABPA with total IgE level to assess treatment response. (C)
Does immunoglobulin replacement treatment therapy improve outcomes in patients with bronchiectasis due to antibody deficiency?
There are no double-blind randomised placebo-controlled trials of immunoglobulin replacement in patients with either primary or secondary antibody deficiency. Cohort studies show that introduction of IgG replacement therapy is associated with a reduced incidence of pneumonia in patients with CVID and XLA.300–303
Randomised controlled trials comparing high dose and low dose intravenous immunoglobulin replacement therapy show that higher doses are associated with reduced incidence of acute sino-pulmonary304 and upper respiratory tract infections.305 Meta-analysis and cohort studies show an inverse relationship between trough IgG levels and rate of serious infections/and or pneumonia in patients with CVID and XLA receiving intravenous IgG therapy.300 306–308
Current guidelines suggest that patients with CVID and bronchiectasis should be treated with an IgG replacement dose of 0.6 g/Kg/month compared with standard treatment of 0.4 g/Kg/month.96 There is however no consensus on the dose of IgG replacement to treat lung disease in patients with primary antibody deficiency or the optimal trough IgG levels to prevent pneumonia and chest infections. North American guidelines for the use of IgG therapy in primary immune deficiency recommend that the goal of therapy should be to improve clinical outcomes rather than aim for a specific trough concentration.309 310
There is no conclusive data to suggest that IgG replacement therapy prevents the progression of bronchiectasis and other pulmonary complication of primary antibody deficiency syndrome. Two longitudinal studies of patients with CVID and XLA on standard IgG replacement doses over 7–8 years showed greater than anticipated annual declines in airflow obstruction and transfer factor.311 312 Two European studies showed that the prevalence of bronchiectasis on CT scan increased over time in patients with primary antibody syndrome on IgG replacement therapy.300 313 The prevalence of bronchiectasis increased from 47.3% to 54.7% in CVID patients and from 33% to 39% in XLA patients over 5 years.300
Evidence statements
Cohort studies and randomised trials of high versus low-dose immunoglobulin replacement therapy in patients with CVID and XLA show a significant reduction in the rate of serious infections including pneumonia. (2++)
IgG replacement therapy may be useful in patients with minor antibody deficiency syndromes (specific polysaccharide antibody deficiency and/or (IgA or IgG subclass) deficiencies with absent/impaired pneumococcal antibodies vaccine responses) who continue to have objective evidence of bacterial sino-pulmonary infection and progressive disease despite appropriate management of bronchiectasis by a respiratory physician and physiotherapist. (2+)
There is no definite data to suggest that IgG replacement therapy prevents onset of bronchiectasis, or delays progression in bronchiectasis. (2+)
Recommendations
Offer IgG therapy to all patients with CVID and XLA. (B)
Consider IgG therapy for patients with specific polysaccharide antibody deficiency and/or IgA deficiency or IgG subclass deficiencies with absent/impaired pneumococcal vaccine antibody responses who continue to have objective evidence of bacterial sino-pulmonary infection and progressive disease despite appropriate management of bronchiectasis. (C)
Good practice points
All patients receiving IgG replacement therapy should be under the joint care of a clinical immunologist and respiratory specialist in bronchiectasis.
Offer patients receiving replacement IgG the choice of hospital or home-based therapy.
Research recommendation
Randomised controlled trials are needed to assess which patients with bronchiectasis would benefit from long term Immunoglobulin G replacement therapy alone or as an adjunct to long term antibiotic therapy- assessing the optimal dose of IgG replacement and identification of ideal trough IgG level to prevent recurrent infections.
Gastro-oesophageal reflux disease (GORD) and Bronchiectasis
There is an association between gastro-oesophageal reflux disease (GORD) and bronchiectasis. An increased prevalence of proximal and distal GORD (40%) was demonstrated by oesophageal monitoring in a cohort of 27 patients with bronchiectasis compared with controls. This finding was not confined to those with severe lung disease, and the detection of pepsin within sputum in this study did not correlate with the finding of GORD.314
Increased severity of bronchiectasis has been observed in patients with significant reflux symptoms. In a cohort study of 163 patients with bronchiectasis, those with reflux symptoms according to the Hull Airways Reflux Questionnaire had a significantly lower FEV1 and a greater number of lobes affected by bronchiectasis on CT scan. There was higher inflammation in sputum and increased chronic colonisation with PPMs. Symptoms of reflux were independently associated with cough severity and exacerbation frequency.98 In another study of 100 patients with bronchiectasis, those patients with upper gastrointestinal symptoms also had a greater number of lobes affected and significantly worse lung function.315
A possible relationship between H. pylori and bronchiectasis symptoms has been described.314 Some studies of H. pylori serology have shown higher levels in bronchiectasis patients compared with control populations. In one study of 100 patients with bronchiectasis measuring specific IgG to H. pylori, seroprevalence was 76% compared with 54.3% of controls. Further analysis showed that those bronchiectasis patients who were defined as sputum producers had significantly higher H. pylori seroprevalence (83.1%) than those defined as non-producers (58.6%). Multiple regression analysis showed an association between H. pylori IgG concentrations (continuous values) and sputum volume and age. Lung function however did not correlate with H. pylori serology in this regression model.316 A further cohort study of 40 patients with bronchiectasis showed H.pylori seropositivity in 75% of patients with bronchiectasis in comparison to 51.5% of healthy control subjects, but there were no significant differences in gastrointestinal symptoms between patients and controls.317 On the other hand Angrill et al failed to find differences in H. pylori seropositivity between bronchiectasis patients and the general population, and studies of bronchial mucosal specimens taken from patients with bronchiectasis did not demonstrate the presence of H. pylori.318
Evidence statement
GORD is common in patients with bronchiectasis and is associated with increased severity of bronchiectasis suggesting a causal relationship (level 2-).
There is a possible association between H. pylori seropositivity and bronchiectasis (2-)
Recommendation
Treat GORD symptoms in patients with bronchiectasis according to existing NICE guidance319. (D)
Good practice points
GORD should be considered in patients with hiatus hernia, persistent coliforms in sputum samples or recurrent exacerbations with no other cause identified.
Investigate patients who may have gastro-oesophageal reflux according to local policies.
Consider the addition of prokinetic agents if symptoms of GORD increase with an airway clearance technique in sitting position. Avoid eating in the hour immediately prior to physiotherapy.
What is the prevalence of rhinosinusitis in patients with stable bronchiectasis and what are the outcomes of treatment?
Chronic rhinosinusitis is defined as persistent upper airway symptoms lasting >12 weeks and can be subdivided by the presence or absence of nasal polyps. The diagnosis of rhinosinusitis is predominantly clinical and made on history and examination with only a limited role for radiology.
Symptoms of rhinosinusitis are very commonly reported in patients with bronchiectasis. In a UK study, 65% of bronchiectasis patients had symptoms of rhinosinusitis (n=95). This was most common in patients with idiopathic disease, affecting 84% of patients.23 In a study of 101 patients with bronchiectasis in Australia, 72% reported symptoms of rhinosinusitis.15
Among patients with upper airway symptoms, Guillemany et al reported that 41.6% had nasal polyps.320 In an unselected bronchiectasis population from Spain (n=91), 80.2% of stable bronchiectasis patients had rhinosinusitis according to EP30S criteria, and 26.4% had nasal polyps.321 Patients with rhinosinusitis may have worse quality of life and worse radiological bronchiectasis than those without rhinosinusitis.322 323
Chronic rhinosinusitis (CRS) can be a feature of idiopathic bronchiectasis, but patients with bronchiectasis and rhinosinusitis should undergo a comprehensive assessment for underlying aetiology as for all patients. Chronic infective rhinosinusitis can be a feature of primary ciliary dyskinesia along with middle ear infections and infertility.
There are no specific randomised controlled trials to guide the management of rhinosinusitis in bronchiectasis. In addition, there is no evidence to demonstrate that treatment of rhinosinusitis will improve respiratory outcomes, such as exacerbation frequency, in bronchiectasis.
In a high proportion of cases, response to treatment for chronic rhinosinusitis is partial and treatments need to be continued over medium to long term. Typical symptoms of nasal polyps include nasal obstruction, hyposmia/anosmia and decreased taste and post-nasal catarrh.
In the absence of specific recommendations and outcome data in bronchiectasis it seems reasonable to follow existing algorithms for the treatment of chronic rhinosinusitis, such as that provided by the European position paper on rhinosinusitis and nasal polyps or the British Society of Allergy and Clinical immunology guidelines.324 325
Nasal irrigation with 0.9% saline is safe, inexpensive and widely used and has been shown to reduce symptoms of CRS, including in patients with CRS and PCD.326 Topic intranasal steroids are the other first line treatment to suppress inflammation in CRS.326 Nasal drops are preferred. Fluticasone and mometasone have the lowest bioavailability and as such as used in preference.327 Macrolides have evidence in the management in chronic rhinosinusitis but are not regarded as first line therapy.328
A proposed algorithm for initial assessment and treatment is shown in figure 5.

{kind=link}
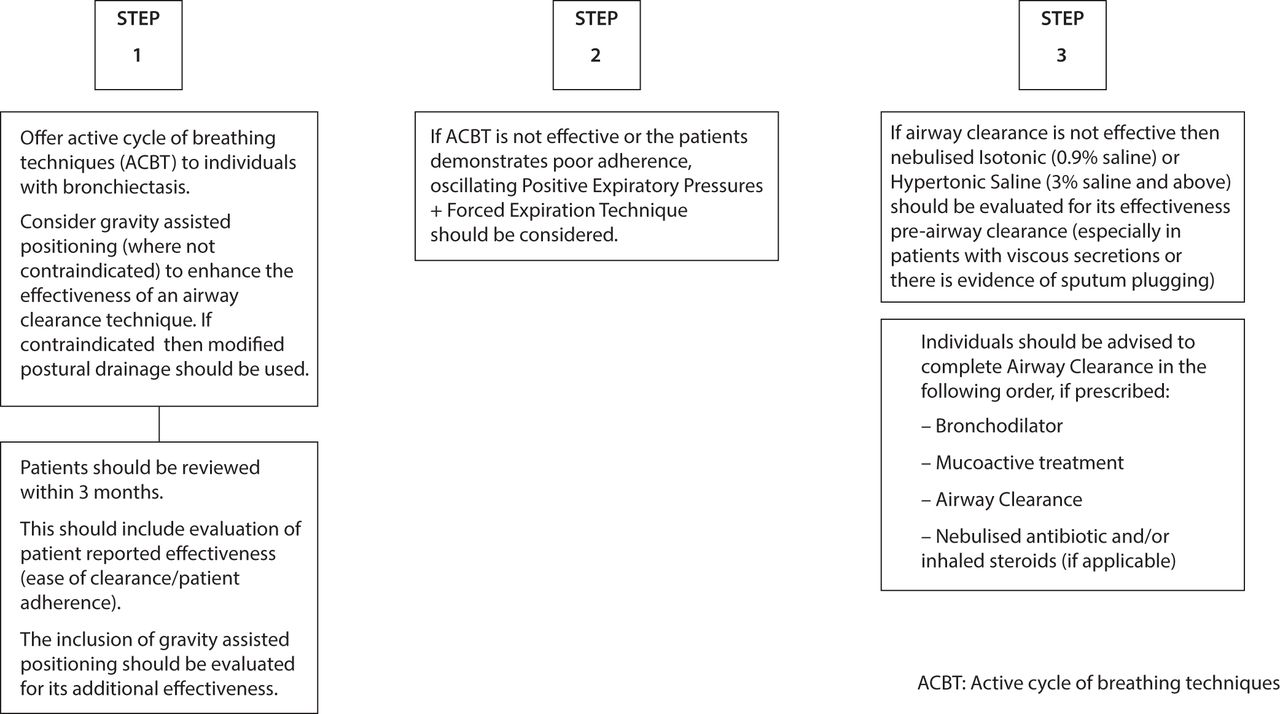{kind=link}
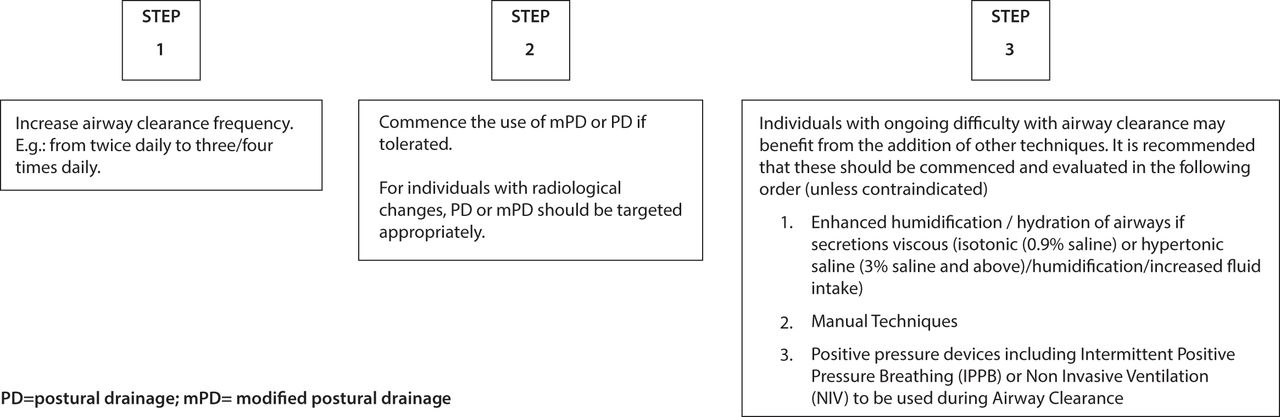{kind=link}
{kind=link}
{kind=link}
Algorithm for initial assessment and treatment - rhinosinusitis.
Sinus CT’s are rarely helpful and reserved for patients failing medical therapy or those with features suggesting alternative diagnoses such as blood stained discharge, displaced globe or severe pain.326
The box above identifies a series of symptoms that indicate an alternative diagnosis, such as orbital symptoms (periorbital oedema, displaced globe, diplopia, ophthalmopegia or reduced visual acuity) severe pain and neurological symptoms. Facial pain without nasal symptoms is rarely due to rhinosinusitis.326
Evidence statements
Chronic rhinosinusitis is common in bronchiectasis and may contribute to impaired quality of life. (2+)
Recommendations
The evaluation of patients with bronchiectasis should include assessment of symptoms of chronic rhinosinusitis. (D)
Patients with bronchiectasis and symptoms of rhinosinusitis should be evaluated and treated according to existing evidence-based treatment pathways. (D)
Should treatment of bronchiectasis be altered in the presence of co-morbidities?
There are no studies addressing treatment of bronchiectasis in the presence of asthma and atopy although an accumulation of clinical experience suggests that these factors need to be addressed for good control of bronchiectasis to be achieved.329 In the presence of this co-morbidity, there is a risk of poor clearance of sputum due to bronchospasm, greater mucus secretion and endobronchial inflammation, all of which is likely to lead to reduction in lung function and poor control of infections.
Several studies have shown a higher than expected prevalence of bronchiectasis in patients with COPD and these patients probably have a worse prognosis than bronchiectasis without COPD; however there is an acknowledged lack of evidence as to implications for treatment.255 269 330–332
Patients with HIV-related disease appear to be at greater risk of bronchiectasis than the general population but management implications were not discussed in the studies reviewed.333 334
Inflammatory bowel disease
The majority of studies are undermined by low numbers, which may reflect the relatively small population of patients with bronchiectasis whose condition is associated with inflammatory bowel disease (IBD) (see online appendix 6 <1%–3%)23 62 Kelly et al studied 10 patients (time period not stated)59 and Mahadeva et al identified 17 patients over a 14 year period with coexistent IBD and pulmonary disease.60 Bronchiectasis appeared to be the most common feature although other abnormalities were seen on CT scan. In some cases a biopsy revealed evidence of lymphocytic inflammation59 and a useful clinical response to oral or inhaled corticosteroids was observed.60 The nature of the steroid treatment and its outcome were not described in detail although alveolitis and bronchiolitis were reported to resolve fully.60
The overlap of IBD and bronchiectasis was comprehensively reviewed in a European Respiratory Monograph in 2011, again with an emphasis on corticosteroid responsiveness although the lack of evidence was acknowledged.335
Rheumatoid arthritis
In a study of the effects of immunosuppression, 37 patients with rheumatic diseases (and nine with IBD) were identified in a database of 539 patients with bronchiectasis: 26 had rheumatoid arthritis (RA).336 The majority developed bronchiectasis after the onset of autoimmune disease. All had received either conventional disease modifying anti-rheumatic drugs (DMARDs) - mostly methotrexate - or biologics. Methotrexate in particular was associated with a range of adverse effects. Patients with RA or IBD were not found to suffer more exacerbations than patients with bronchiectasis alone, and the frequency of colonising organisms such as P. aeruginosa and H. influenzae was similar. Longitudinal data were available for a small cohort of patients with RA and bronchiectasis. In these patients, control of RA disease activity appeared to track with spirometry, in that spirometry declined when the DAS score rose, and vice versa. DMARDs did appear to be associated with increased pneumonia and other infections.
The risk of infection in patients using DMARDs or biologics was assessed in a cohort of >3000 patients, of whom 86 had both a rheumatological disease and bronchiectasis.337 Sufficient data was available on only 47 patients receiving DMARDs or biologics. Of 40 patients with RA and bronchiectasis, 35 were seropositive. 13 had bronchiectasis prior to RA, 27 were diagnosed with bronchiectasis after the onset of RA but it was attributed directly to RA only in 13 cases, otherwise the aetiology was thought to be childhood infection. An OR of 8.7 (95% CI 1.7 to 43.4) was found for respiratory infections in patients treated with biologics compared with traditional DMARDs. The OR for infections was 7.4 (2.0–26.8) in the presence of previous sputum colonisation by potentially pathogenic micro-organisms. The authors therefore recommended using non-biologics in preference to biologics if possible. Etanercept and rituximab were associated with a lower rate of infections than the other biologics, but the numbers were very small in this study.
Evidence statements
Patients with bronchiectasis and comorbid COPD have more severe disease and worse prognosis than those with bronchiectasis alone. (2+)
Patients with co-morbid rheumatoid arthritis and bronchiectasis may have worse outcome than those with either disease alone. (3)
Immunosuppressive treatment for connective tissue disorders is associated with a higher risk of infection in general; biologics may promote infections more than traditional DMARDs, and the risk may be higher in patients already colonised with potentially pathogenic micro-organisms. (3)
Inflammatory bowel disease-related bronchiectasis may be responsive to corticosteroids. (3)
Recommendations
Consider a trial of inhaled and/or oral corticosteroids in patients with bronchiectasis and IBD. (D)
Ensure optimal control of asthma and allergies in patients with both bronchiectasis and asthma (D).
Monitor patients with co-morbid COPD and bronchiectasis as they are at higher risk of death. (D)
Patients with bronchiectasis and autoimmune conditions should be carefully assessed for autoimmune related lung disease and often require long term follow-up in a secondary care setting. (D)
Patients with bronchiectasis who require DMARDs or biologics for rheumatoid arthritis should be referred to a chest physician for further assessment before treatment is started. (D)
Section 15
How should we monitor bronchiectasis?
There are no studies in bronchiectasis comparing different monitoring schedules, or relating particular monitoring strategies to clinical outcomes. Factors associated with increased risk of exacerbations, hospitalisations and mortality in bronchiectasis include age, body mass index, past history of exacerbations and or hospitalisations, persistent infection, especially with P. aeruginosa, dyspnoea as measured on the MRC scale, radiological extent of disease and airflow limitation (FEV1) (see tables 6 and 7). These components have recently been operationalised into two multi-component scores BSI120 and FACED.119 Recently a comparative analysis has suggested BSI has greater sensitivity in predicting those at risk of future risk of exacerbations.121 In addition, co-morbidities such as COPD and rheumatoid arthritis have also been shown to affect mortality and therefore should be recorded.269 338 The role of the bronchiectasis aetiology and comorbidity index (BACI) in routine practice is yet to be determined.338
It seems reasonable to propose that routine monitoring should include reassessment of the variables above that have been shown to be relevant in bronchiectasis. In addition patient monitoring should include assessment of symptoms and the impact that these have on health status. This may be best achieved using a validated tool, of which there are many,339 including tools specifically for bronchiectasis such as the QOL-B.340 Systematic review has demonstrated that these tools may assess components of health status in bronchiectasis not measured using other outcomes.339 Routine monitoring of quality of life may not be needed in all cases but should be considered when higher cost interventions are planned. The optimal tool for monitoring treatment effects has however yet to be determined in bronchiectasis. As in other respiratory disease, exercise capacity can be assessed using 6MWD or ISWT and even small changes in these measures may reflect important changes in health.221
The BTS Quality Standards for clinically significant bronchiectasis in adults 2012,341 based on the 2010 BTS guideline for non-CF bronchiectasis, suggested that patients fulfilling the following criteria should continue to receive specialist input in secondary or specialist care. The guideline development group advise using the following criteria:
patients with chronic P. aeruginosa, non-tuberculous mycobacteria or methicillin-resistant S. aureus colonisation (MRSA);
deteriorating bronchiectasis with declining lung function;
recurrent exacerbations (≥3 per year);
patients receiving long term antibiotic therapy (oral, inhaled or nebulised);
patients with bronchiectasis and associated rheumatoid arthritis, immune deficiency, inflammatory bowel disease and primary ciliary dyskinesia;
patients with allergic bronchopulmonary aspergillosis;
patients with advanced disease and those considering transplantation.
Evidence statement
Variables exist which affect outcome in bronchiectasis and such variables can be monitored over time.119 120 (1+)
No studies have however measured the impact of such monitoring, or demonstrated that action taken in response to changes in measured variables will affect outcome.
Recommendation
All patients with bronchiectasis should undergo routine monitoring in order to identify disease progression, pathogen emergence and modify treatment where necessary. (D)
Good practice points
Tailor the frequency of routine monitoring to the patient’s disease severity (see table 7).
Assess patients annually, and more frequently in more severe disease.
Perform pulse oximetry to screen for patients who may need blood gas analysis to detect respiratory failure.
A baseline CXR may provide a useful comparator in the event of clinical deterioration.
Section 16
Is there a role for microbiological sensitivity testing?
Evidence summary
Despite widespread use of sensitivity testing to inform antibiotic treatment in patients with bronchiectasis, there are no published RCTs which determine whether antibiotic treatment guided by antibiotic sensitivity results improve clinical outcomes for patients.
RCTs suggest that acute antibiotic treatment rarely results in the development of resistance. For example, Bilton et al reported that P. aeruginosa resistance to tobramycin developed in only 1/27 patients receiving oral ciprofloxacin and tobramycin inhalation solution for 14 days.285 Likewise, Barker et al reported that only 4/36 (11%) patients receiving tobramycin inhalation solution for 4 weeks who began the study with susceptible P. aeruginosa had resistant P. aeruginosa at their last visit.342
Long term inhaled antibiotic treatment only occasionally results in the development of resistance. For example, Murray et al reported that resistance to gentamicin did not develop in 57 patients receiving either nebulised gentamicin or placebo for 1 year.201 Similarly, Drobnic et al reported that in a study assessing the efficacy of 6 month tobramycin inhalation therapy in 30 patients, resistant P. aeruginosa was only detected in sputum from two patients during the tobramycin treatment period.343 Equally, in an RCT comparing treatment with inhaled colistin (n=73 participants) or placebo (n=71 participants) for up to 6 months in patients with chronic P. aeruginosa infection, no colistin–resistant strains of P. aeruginosa were identified and there were no significant differences in treatment-emergent pathogens between treatment groups.200
There has also been considerable focus on the development of resistance with long-term oral treatment with macrolides. In a meta-analysis assessing the clinical effect of long-term macrolides in bronchiectasis,196 two studies included reported on emergence of macrolide resistance: Altenburg et al reported that during treatment, 53 of 60 pathogens (88%) tested for sensitivity in 20 patients in the azithromycin group became macrolide resistant compared with 29 of 112 pathogens (26%) in 22 patients in the placebo group (P<0.001 by t-test).191 Serisier et al reported erythromycin significantly increased the proportion of macrolide-resistant commensal oropharyngeal streptococci (P<0.001).192 However, a meta-analysis was not possible due to the diversity of parameters. Resistance development following long-term treatment with quinolones has also been assessed; Rayner et al 1994344 reported that, following continuous treatment with oral ciprofloxacin for at least 90 days, resistance to ciprofloxacin developed in two patients with P. aeruginosa infection and this was associated with clinical deterioration.344
A laboratory based study has questioned the use of current susceptibility testing methods for the complex populations of bacteria found in chronic lung infection. Gilham et al used the disc diffusion method to determine the minimum inhibitory concentration (MIC) of multiple P. aeruginosa morphotypes isolated from sputa from patients with bronchiectasis.345 There was considerable variation in inhibition zone size between multiple colonies of the same morphotype with the range of zone sizes crossing the breakpoint between resistance and susceptibility in 11/33 samples analysed. This clearly highlighted that sensitivity testing in bronchiectasis is likely to be poorly reproducible with the result depending on the particular colonies tested.
Evidence statements
There is no evidence to show that antibiotic treatment guided by sensitivity results improves clinical outcomes for patients.4
Acute antibiotic treatment only occasionally results in the development of resistance. (1-)
Long-term macrolide use results in the emergence of macrolide resistance. (1-)
Good practice points
Antibiotic sensitivity testing can be used to determine if resistance develops to either acute or long-term antibiotic treatment.
Where possible, treatment should be guided by antibiotic sensitivity results but is often empirical based on previous sputum bacteriology.
Some patients with an infective exacerbation may respond to antibiotic treatment despite resistance to that drug in vitro. Antibiotics should only be changed if there is no clinical response.
For those on long term antibiotic treatment, there should be repeat sensitivity testing where there is a clinical concern regarding loss of efficacy with therapy.
Section 17
Is there any evidence of cross-infection with pathogenic organisms (conventional bacteria and environmental mycobacteria)?
While there are numerous studies confirming the transmissibility of certain epidemic strains of P. aeruginosa and more recently Mycobacterium abscessus (M. abscessus) in cystic fibrosis (CF) there are few studies assessing the potential for cross-infection in bronchiectasis.346 347 The available studies of cross infection in bronchiectasis are mostly single centre design, often focus on P. aeruginosa, and have relatively limited longitudinal sampling with often limited description of the clinical setting.348 349 This latter aspect may be particularly important if facilities are shared with patients who have CF and carry known CF epidemic strains.
De Soyza et al reported a case series of 40 patients from a single adult bronchiectasis clinic in Newcastle, UK, not practising strict segregation but with reported limited sharing of facilities with CF patients.348 The study focused on P. aeruginosa. It was a predominantly cross- sectional design although it reported longitudinal follow-up of 10 patients for up to 4 years. Their data suggested no single common ‘epidemic strain’ was found. They identified however that certain common strains that are found widely within the natural environment for example, Pseudomonas Clone C can be found in patients attending bronchiectasis clinics. This raises the potential for environmental acquisition in the bronchiectasis population.
Pujana et al similarly used a single centre, short-term study using bacterial fingerprinting using a PCR approach.349 In this study of 16 patients with bronchiectasis from Bilbao, Spain, 64 P.aeruginosa isolates were examined. Cross-infection or common source acquisition did not appear to have occurred. A study of 125 isolates taken from 31 patients attending two clinics in Spain using pulsed field gel electrophoresis suggested certain strains may be predominant within a clinic.350
Two papers which have used the higher resolution of whole genome sequencing (WGS) have raised the possibility of cross infection. A summary of studies to date would support the conclusion that significant cross infection with P. aeruginosa has not been identified, but longitudinal studies are needed.351 352
One study has suggested potentially similar clones of Mycobacterium avium (M. avium) are present in patients with chronic lung disease.353 The study included some patients with bronchiectasis though confirming the exact number was not possible. The study aims were primarily to compare the benefits of VNTR fingerprinting over PFGE, the present ‘gold standard’ to allow a worldwide database. This aim was achieved. The authors noted different patients’ isolates had the same VNTR types and these were mostly clonal by PFGE suggesting that clonal groups do exist with M. intracellulare. Despite this evidence, the authors provided no evidence or discussion on the question of transmission of M. avium. There are therefore inadequate data to provide a definitive statement on the risk of M. avium transmission in bronchiectasis. There are no extensive data on M. abscessus infection in bronchiectasis but this is a rapidly changing field.
Evidence statements
There is no evidence of transmissibility of epidemic P. aeruginosa in the available cohort studies. (2-)
There is no evidence of transmissibility of M. avium in the available cohort studies. (2-)
Recommendation
Individual or cohort segregation based on respiratory tract microbiology results is not routinely required for patients with bronchiectasis. (D)
Good practice points
Good cross infection prevention principles should be applied: seek advice on local policies.
The transmissibility of P. aeruginosa in cystic fibrosis appears more common. In the case of shared facilities with cystic fibrosis patients the cross infection guidelines for cystic fibrosis should prevail.
Research recommendation
Large scale robust data that confirm or refute the transmissibility of key pathogens such as P. aeruginosa and non-tuberculous mycobacteria are needed.
Section 18
Specialist vs non-specialist setting
There are no studies available describing differences in outcome for patients with bronchiectasis in specialist compared with non-specialist care settings. The consensus team (expert opinion) suggest there may be benefits to patients by attending a specialist clinic for bronchiectasis as this will facilitate access to appropriate diagnostic and management expertise through a multidisciplinary team (for example Respiratory Nurse Specialists, Pharmacists, Consultants with a special interest in bronchiectasis, Immunology Consultants, Respiratory Radiologists, Dieticians and Psychologists). This may be most relevant to patients with severe or complex disease.
Good practice point
Specialist clinics should be considered in patients requiring hospital follow-up.
Section 19
What are the complications of bronchiectasis?
Complications of bronchiectasis may have changed over the years. Haemoptysis and thoracic infections have always been important, but finger clubbing and metastatic infection such as cerebral abscesses are now rare.15 354
Chronic respiratory failure
Most patients with bronchiectasis have some degree of lung function impairment, but lung function decline over time was only slightly greater than normal in a follow-up study of patients in Edinburgh.355 Lung function was shown to be capable of improvement as well as decline in a UK study focusing on potential impact of P. aeruginosa colonisation in patients with bronchiectasis.274 An Australian study linked risk of decline with higher volume of daily sputum at baseline.15
A recent analysis of patients recorded on the EMBARC European bronchiectasis database revealed that 86 of 1145 (7.5%) patients were using long term oxygen therapy for chronic respiratory failure. 356
Haemoptysis
A series at the Mayo Clinic from 1976 to 1993 identified 3421 patients seen for bronchiectasis, of whom 134 patients underwent pulmonary resection.357 Haemoptysis was present in 63 of the lung resection group, and was the indication for surgery in 26 (19.4%). The frequency of haemoptysis in medically managed patients was not given.
One study from Korea has suggested that use of inhalers may increase the risk of haemoptysis358.
The degree of haemoptysis can vary widely. Streaks of haemoptysis can be seen with chest infections and sometimes in stable patients with severe bronchiectasis who are treated with anti-platelet therapy or anti-coagulant therapy for comorbid conditions.
The volume of blood defining major haemoptysis is not known, with no internationally agreed definition.
Good practice point
If haemoptysis 10 mls or less over a 24 hour period, treat with an appropriate oral antibiotic. If clinical deterioration, arrange emergency admission to hospital.
Management of major haemoptysis should be multidisciplinary with involvement of respiratory physicians, interventional radiology and thoracic surgeons. Empirically treat patients with intravenous antibiotic therapy, based on their known microbiology, and consider adjunct treatment with tranexamic acid. Bronchial artery embolisation is the recommended first line treatment if significant haemoptysis persists.
Chest pain
Chest pain is reported in studies of symptoms of bronchiectasis, but not often well described. King et al prospectively assessed chest pain experienced by 1787 patients with bronchiectasis over a 8 year follow-up period at the Monash Medical Centre.359 A careful assessment of the nature of the pain was made to test the hypothesis of visceral pain sensation related to bronchial inflammation. This bronchiectasis population was comparable to the UK population, except that a smaller proportion in Monash (43/178) were taking inhaled corticosteroids than is suggested by the results of previous UK BTS bronchiectasis audits.166 360 44 of the patients reported chest pain, and for 39 of these, the pain was associated with exacerbations. Only four had clear pleuritic pain, and 37 had other types of pain, with two having both pleuritic and other pain. The pain did appear to co-localise with the position of bronchiectasis on CT scan. It did not appear musculoskeletal related to coughing and was not associated with chest wall tenderness. It tended to occur early in the course of an exacerbation, and subside only towards the end of the recovery period. In 18 out of 33 patients who had imaging at the time of an exacerbation associated with chest pain, there were abnormalities such as consolidation, collapse or atelectasis. Only 13 subjects reported retrosternal discomfort associated with visceral airway pain receptors.
Lung cancer
A case series of post mortem specimens of 20 smokers and ex-smokers with peripheral nodular carcinoma of the lung showed that in 16 out of 20 cases the neoplasia arose out of clusters of non-segmental bronchiectasis.361 A database study of 57 576 patients hospitalised with bronchiectasis between 1998 and 2010 in Taiwan showed an increased risk of lung cancer compared with a cohort of 2 30 304 patients without bronchiectasis, adjusted for age, sex and comorbidities (adjusted HR=2.36, 95%CI=2.19 to 2.35).362 Conversely a case-control study in South Korea of patients with moderate to severe COPD and lung cancer found that bronchiectasis was less prevalent in the patients with lung cancer than in matched controls without lung cancer (OR 0.25, 95% CI 0.12 to 0.52), suggesting that the disease process in bronchiectasis may not increase the risk of lung cancer.363
Vascular complications
In a primary care database study, the rate of first coronary heart disease (CHD) and stroke were higher in people with bronchiectasis (HR for CHD 1.44 (95% CI 1.27 to 1.63) and HR for stroke 1.71 (95% CI 1.54 to 1.90)).364
Bronchiectasis severity (moderate or worse) has been shown to be an independent risk factor for vascular disease,365 with recurrent exacerbations (three or more per year) showing increased aortic stiffness.366
A retrospective UK study examined the CT scans of 91 patients with bronchiectasis previously recruited for a quality of life study, and inferred the presence of pulmonary hypertension from measurement of the pulmonary arteriesand found there was an increased risk of death (HR, 1.24; 95% CI, 1.13 to 1.35; P<0.0001) in the presence of pulmonary hypertension in this study.367
Severe pulmonary hypertension was found in 12 patients from a prospective cross sectional study in Saudi Arabia of 94 patients with bronchiectasis but no known cardiac disease or cardiac risk factors, all with cystic bronchiectasis. Poorer ventilatory function was associated with increased risk of pulmonary hypertension.368
Other
In patients with bronchiectasis, depression and anxiety do occur at higher rates than in the healthy population.369–371 In a British study, there was a link between depression and exercise limitation due to breathlessness.369 In a Spanish study, using the Beck Depression Inventory and the State-Trait Anxiety Inventory, 34% of patients had depression, 58.1% were above the 50th percentile for state anxiety and 56.8% were above the 50% percentile for trait anxiety. 30% of patients had both anxiety and depression. Anxiety showed some correlation with sputum volume and bacterial colonisation, particularly P. aeruginosa, while depression appeared more common in women.372 A Korean study did not identify a link between mood disorders and specific clinical features of bronchiectasis.371
An important finding from an uncontrolled cross sectional study of 76 women attending a specialist bronchiectasis clinic in Newcastle-upon-Tyne was that 55% of women had symptoms of urinary incontinence.373
A study of systemic comorbidities included assessment of bone mineral density, which was not significantly different in patients with bronchiectasis and healthy controls matched for age, sex and smoking status.374
Corticosteroid responses in patients with bronchiectasis, of whom a high proportion were taking inhaled fluticasone, were found to be impaired in a cross-sectional analysis.176 Inhaled fluticasone treatment appeared to double the risk. Adrenal insufficiency was associated with poorer quality of life. This issue was addressed more fully in a case-control study of subjects with bronchiectasis and age- and sex-matched healthy controls, who were all subjected to low dose short synacthen tests.375 One patient with post-tuberculous bronchiectasis had absolute adrenal insufficiency and was treated with steroid replacement. In 38 patients with a valid baseline result, 15 had an impaired response to one microgram cosyntropin. The response was significantly better in controls, and was not affected by maintenance treatment with budesonide.
Nutritional deficiency has been noted incidentally in various studies376 and was studied specifically by Olveira et al, but this study included both CF and non-CF bronchiectasis, which limits its applicability to this guideline.377
Fatigue and reduced exercise tolerance are commonly reported in bronchiectasis. In a UK study of 117 consecutive patients, routine clinical assessment included lung function, MRC dyspnoea score, sputum microbiology and an assessment of fatigue on the fatigue impact scale (FIS).378 Significant fatigue was found in 45% and was positively correlated with the MRC score (r=0.57, P<0.001) and negatively correlated with FEV1 % predicted (r=−0.30, P=0.001). An Australian study identified fatigue in 74% of 103 patients with bronchiectasis.379
Section 20
Summary of research recommendations
See appendix 8 for details of the research recommendations in PICO format.
Consensus criteria for diagnosis of ABPA need to be validated in bronchiectasis cohorts.
Consensus criteria for definition of abnormal post pneumococcal test immunisation antibody responses need to be validated in bronchiectasis cohorts.
Randomised controlled trials using clinically important outcome measures are required to assess the effectiveness of airway clearance techniques in varying severities of bronchiectasis.
Randomised controlled trials are required to evaluate the effects of airway clearance techniques in patients who are undergoing an exacerbation.
Randomised controlled trials are needed to assess the long term impact of muco-active therapies.
Randomised controlled trials are needed to assess the long term impact of anti-inflammatory therapies.
Long term randomised controlled trials of oral and inhaled antibiotics are needed to assess their efficacy and safety in patients with bronchiectasis who have frequent respiratory tract infections with recurrent P. aeruginosa infection or other potential pathogenic micro-organisms.
Further interventional/randomised controlled trials needed to establish the role of any alternative therapies in the management of bronchiectasis.
Studies assessing the benefits of nutritional supplementation in patients with bronchiectasis should be undertaken.
The role of education, self management plans and who delivers the pulmonary rehabilitation needs to be explored.
The role of pulmonary rehabilitation after exacerbations requiring hospital admission needs to be explored.
The incidence of cross-infection of respiratory pathogens in the group exercise setting should be investigated in the bronchiectasis population.
A randomised control trial of P. aeruginosa eradication therapy is needed to determine the microbiological and clinical outcomes of eradication therapy.
Randomised controlled trials are needed to assess which patients with bronchiectasis would benefit from long term Immunoglobulin G replacement therapy alone or as an adjunct to long term antibiotic therapy- assessing the optimal dose of IgG replacement and identification of ideal trough IgG level to prevent recurrent infections.
Large scale robust data that confirm or refute the transmissibility of key pathogens such as P. aeruginosa and non-tuberculous mycobacteria are needed.
Acknowledgements
Guideline Development Group members are grateful to the members of the BTS Standards of Care Committee for their assistance during the production of the Guideline.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
Contributors ATH, ALS and MRL chaired the guideline group, and as lead author led the drafting and revision of the document. All authors drafted sections of the guideline and undertook revisions of the paper. ATH, ALS and MRL had final responsibility for the guideline.
Competing interests All authors have completed a declaration of interest form in line with BTS Policy and copies are available from BTS head office on request. JDC has declared funding from Bayer Healthcare, Griffols, Pfizer, Insmed, Chiesi, Boehringer Ingelheim, GlaxoSmithkline, Astra Zeneca, Napp. ADS has declared funding from Bayer Healthcare, Pfizer, Insmed, Boehringer Ingelheim, Astra Zeneca. SE has declared funding from GlaxoSmithKline. AF has declared funding from GlaxoSmithKline, Zambon, Insmed, Verona. KGJ has declared funding from Boehringer Ingelheim, GlaxoSmithkline, Astra Zeneca, Napp, TEVA, Chiesi, Nutricia, Novartis. CSH has declared funding from Aradigm, Gilead, Griffols, Insmed, Chiesi, GlaxoSmithkline, TEVA, Vertex, Zambon, Novartis. ATH has declared funding from Bayer Healthcare, Boehringer Ingelheim. JRH has declared funding from Pfizer. MRL has declared funding from Bayer Healthcare, Insmed, Pulmocide, Griffols, Polyphor, Savara. MT has declared funding from Novartis, Basilea, Stragen. RW has declared funding from Bayer Healthcare.
Patient consent Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves