Article Text

Statistics from Altmetric.com
Although there is evidence that patients with obstructive sleep apnoea (OSA) have anatomical susceptibility coupled with abnormalities in upper airway motor control and/or instability in ventilatory control, the data now suggest that the mechanisms underlying OSA vary considerably between patients.1 In some patients OSA is primarily the result of anatomical problems, while in others it may be due to dysfunctional motor control with only minimal anatomical abnormality. Similarly, abnormal ventilatory control (loop gain) may be important in only a subgroup of patients with OSA.2 As a result, the concept of individualised therapy has now emerged, such that treatment of the major underlying abnormality is likely to be beneficial in the appropriately targeted patient subgroups.3 In theory, patients with OSA who respond well to palatal surgery probably primarily have an abnormality in the velopharyngeal anatomy,4 whereas those who respond well to oxygen may have mainly an abnormality in ventilatory control instability.5 6
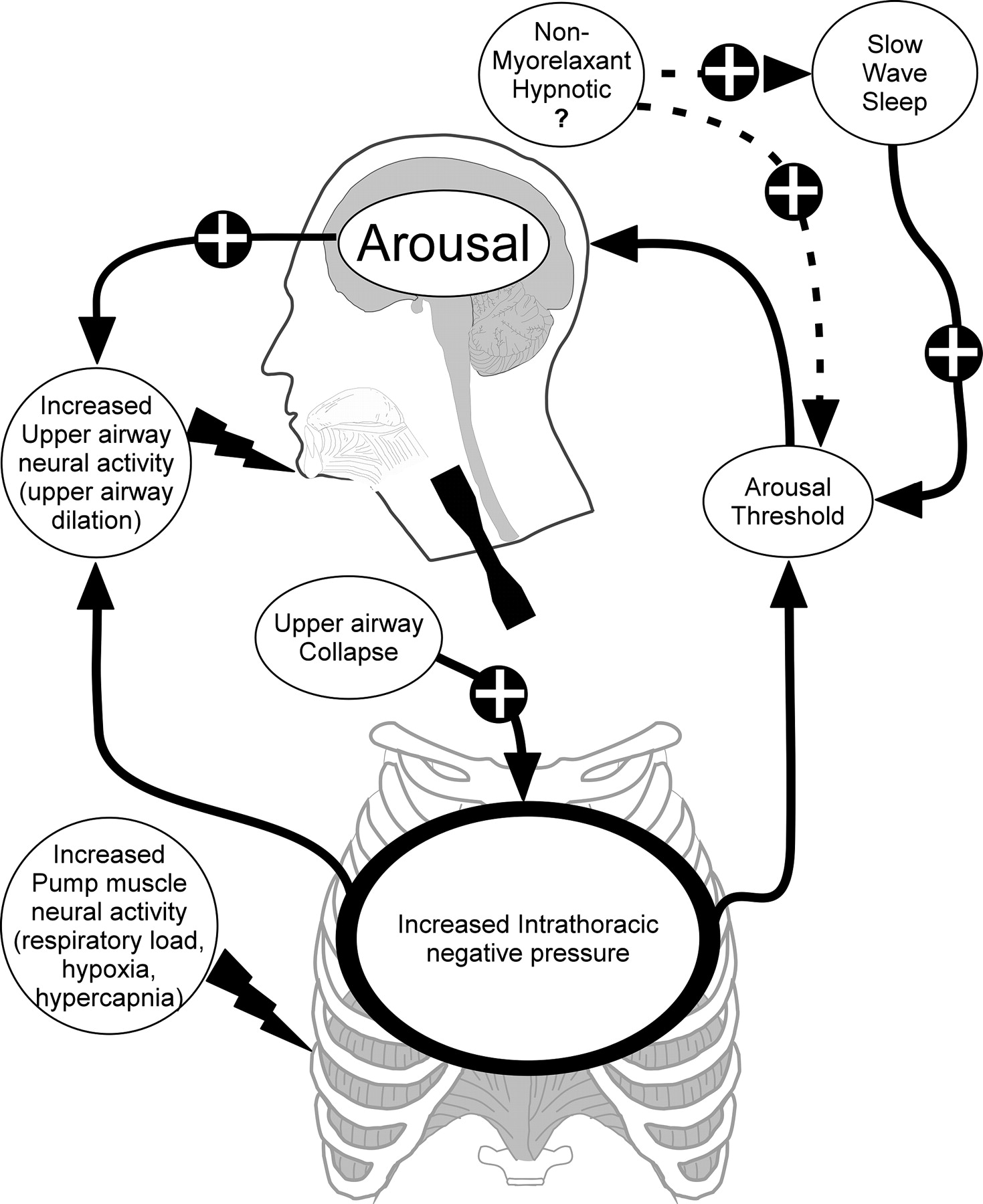
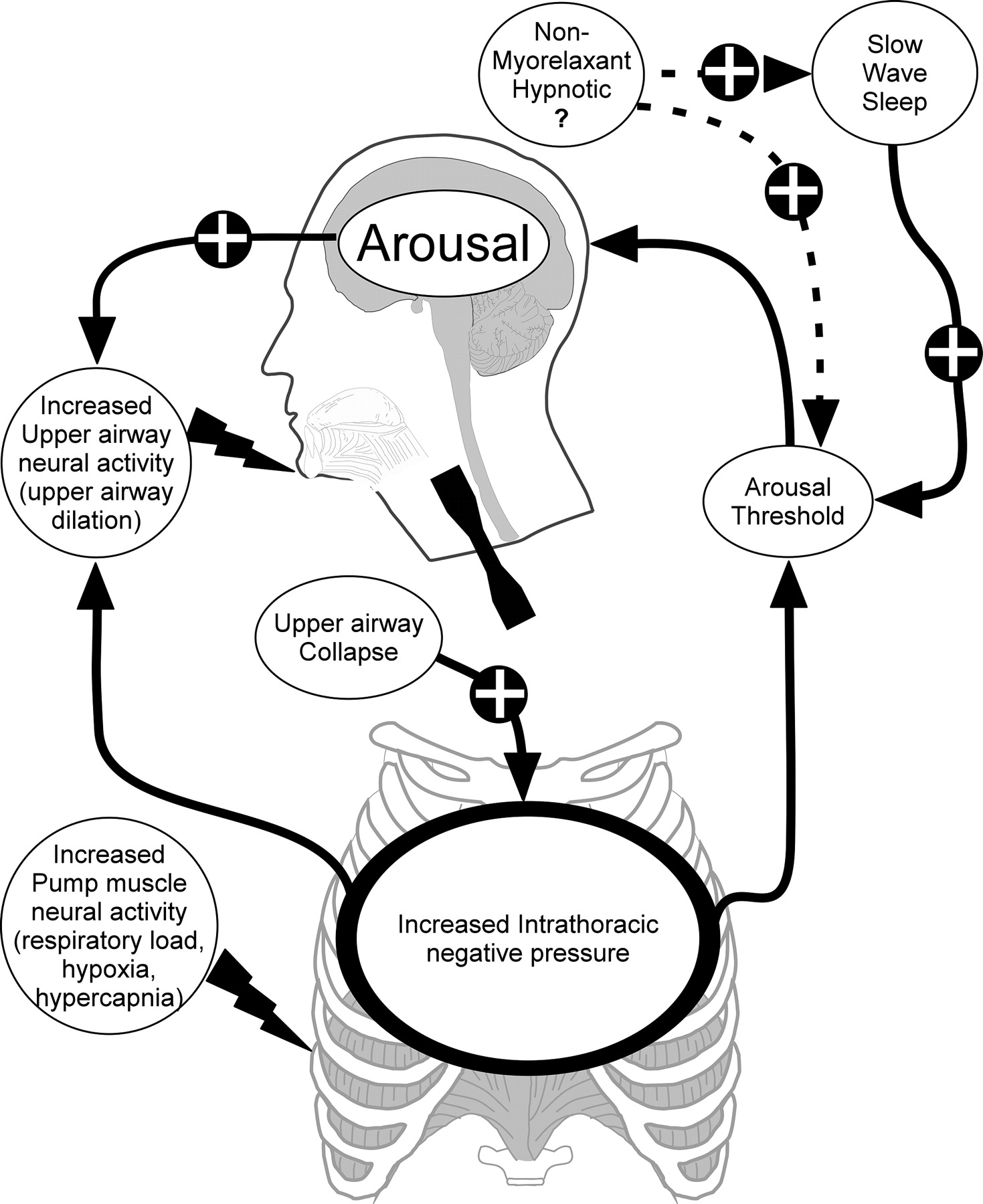
The arousal threshold is one concept that has received some—but not sufficient—attention in the OSA arena.7 8 The trigger for arousal from sleep during respiratory events is believed to be increasing negative intrathoracic pressure9 (see figure 1). The realisation of the importance of the arousal threshold in the pathogenesis of OSA has recently been brought to light by the work of Younes, particularly the emphasis that most patients with OSA spontaneously have some periods of stable breathing.10 11 Jordan et al recently observed that these stable breathing periods were associated with markedly increased activity in the genioglossus, suggesting that upper airway dilator muscles are necessary and sufficient to stabilise the upper airway with endogenous stimuli.12 Upper airway muscles are known to have robust responsiveness to respiratory stimuli including CO2 (through chemoreceptors) and through intrapharyngeal negative pressure (via mechanoreceptors) during wakefulness.13 14 Recent single motor unit studies of the genioglossus suggest that recruitment is likely to be mediated through activity in additional motor units rather than significant increases in motor unit firing frequency, although further work is required in this area.15 However, during sleep the responsiveness of these muscles is considerably attenuated compared with wakefulness, such that more marked stimuli for greater duration are required to achieve upper airway muscle recruitment.16 Because accumulation of respiratory stimuli takes time to occur during sleep, the arousal threshold becomes a critical variable—that is, premature arousal from sleep may lead to repetitive apnoea due to inadequate accumulation of respiratory stimuli to activate upper airway muscles. On the other hand, a very high arousal threshold (hard to wake up) may be deleterious if profound hypoxaemia and hypercapnia occur before arousal. Thus, manipulation of the arousal threshold may be beneficial for some patients (those with a low arousal threshold but recruitable upper airway muscles) (figure 1) but deleterious for others (in whom deterioration in blood gases leads to end organ damage).
{kind=link}
Schematic representation of the chain of events that leads to arousal in obstructive sleep apnoea and possible modulating factors. The stimulus to respiratory load-induced arousal is believed to be increased respiratory effort (increased intrathoracic negative pressure). In the case of obstructive sleep apnoea, this is typically associated with hypoxia or hypercapnia. These stimuli provide additional neural output to the respiratory pump and upper airway dilator muscles. The termination of an apnoea or hypopnoea generally requires arousal from sleep. However, if upper airway dilator muscle activity increases sufficiently to re-establish pharyngeal patency, the event may be terminated without an arousal and thus less sleep fragmentation. Slow wave sleep increases the arousal threshold, thus potentially providing additional time for the upper airway muscles to respond sufficiently to overcome the collapsed pharynx. Non-myorelaxant hypnotics may directly increase the arousal threshold or slow wave sleep and promote stable breathing (proposed pathways indicated by dotted lines). In selected patients (with a low arousal threshold), this pharmacological approach may be beneficial. The plus sign indicates increased input to the selected pathway. Some arrows have been deleted for clarity.
Several points are worthy of emphasis from the standpoint of arousal. First, recent studies have shown that the increase in arousal threshold seen in patients with OSA is probably acquired (at least in part) rather than intrinsic to the disease.17 Thus, with continuous positive airway pressure (CPAP) the arousal threshold in OSA is lowered, suggesting that the increase in arousal threshold is probably an adaptive response which occurs over time in response to sleep fragmentation and/or hypoxaemia. Second, certain hypnotic agents can raise the arousal threshold and are likely to be beneficial for carefully selected patients with OSA18 (figure 1). Third, when arousal occurs, there is a robust ventilatory response which itself can be destabilising.19 If the ventilatory response to arousal is sufficiently marked, it can drive the arterial carbon dioxide tension below the chemical apnoea threshold, leading to either central or obstructive apnoea depending on the prevailing upper airway mechanics. Of note, many techniques that assess ventilatory instability rely on stable state (no arousals), such that the impact of the ventilatory response to arousal is frequently overlooked.20
In this issue of Thorax, Ratnavadival et al21 provide an important insight into several critical questions (see page 107). The authors have observed an increase in arousal threshold to respiratory stimuli in slow wave sleep (SWS) compared with stage 2 non-REM sleep. This concept has been minimally studied but is consistent with changes observed between stage 2 and SWS in healthy men in response to occlusion stimuli.22 A separate study reported data for minimal oesophageal pressure before arousal during naturally occurring events in light sleep (stages 1 and 2) and SWS in patients with severe OSA.23 However, no direct comparisons were made and subject numbers differed, precluding retrospective comparison of these data between light sleep and SWS. Thus, the observations by Ratnavadival et al help answer an age-old question as to why SWS is stabilising from the standpoint of breathing. While some have argued that SWS only occurs when breathing is stable, others have suggested that SWS per se stabilises breathing. The observation that SWS is associated with an increase in arousal threshold might suggest that patients with OSA experience stable breathing due to an accumulation of respiratory stimuli rather than SWS being simply a marker of stable breathing. Some but not all studies have shown increased phasic upper airway muscle activity in SWS compared with other non-REM stages.24 The new findings have important clinical implications and might suggest that, if a high arousal threshold could be achieved pharmacologically, a stable breathing pattern may be predicted. Such an approach would have to be undertaken cautiously since the selection of patients and the appropriate agent for this approach would be critical. In theory, a non-myorelaxant hypnotic would be predicted to stabilise breathing if given to patients with a low arousal threshold but with recruitable upper airway muscles (figure 1). Alternatively, certain agents have been reported to induce SWS (eg, sodium oxybate,25 thalidomide, high-dose trazodone26), and they may also theoretically provide benefits from the standpoint of breathing. However, blinded randomised trials will clearly be required to determine whether these strategies actually improve clinical outcomes. In theory, the markedly negative intrathoracic pressure seen during stable flow limited breathing may represent a substantial afterload on the left ventricle.27 28 Such an afterload effect could potentially outweigh the benefits of reducing hypoxaemia and arousals in certain patients. Ultimately, genetic and other biomarkers may be required to determine to which physiological stress a given individual may be most susceptible and from what pharmacological strategy an individual may benefit.
References
Footnotes
Linked articles 112953.
Competing interests None.
Provenance and peer review Commissioned; not externally peer reviewed.