Article Text

Statistics from Altmetric.com
History
BONE CHANGES
Even before the introduction of X-rays, Besnier1 had noted the association of swelling of the fingers with lupus pernio. In 1904 Karl Kreibich, later Professor of Dermatology in Prague but at that time working in Vienna, described four patients with cystic changes in the bones of the hand in connection with lupus pernio and gave an excellent radiographic reproduction of the hands in one and sarcoid histology of the skin in another.2 Other reports showing bone involvement by sarcoidosis were published soon thereafter.3-6 In 1919 Schaumann5 was the first to emphasise the location of the specific granuloma in the marrow. The first detailed accounts of the radiology were those of Fleiscner7 and Jungling8 who demonstrated that radiological involvement is more frequent in the bones of the hands and feet than in the long bones, vertebrae, or skull. James9 in 1959 was the first to recognise that bone involvement occurs very rarely in the absence of skin lesions but is common in patients with persistent disease, especially with lupus pernio and other skin lesions.10 The first study on trabecular osteoporosis in 49 untreated patients was possible only when computed tomography became available11; our group has shown that a mild trabecular bone loss may appear only in chronic sarcoidosis. This feature had never been noted before because simple radiographic studies are not sensitive enough to show a mild osteoporosis and because there is rarely an indication for biopsy of the bone affected by sarcoidosis. Our findings have been confirmed by two other groups.12 ,13
Corticosteroids may, of course, cause osteoporosis14 which is spontaneously reversible, at least in young people, if the treatment can be discontinued for at least six months.15
CALCIUM METABOLISM CHANGES
Hypercalcaemia in sarcoidosis was first demonstrated in 1939.16 The next milestone was the discovery in 1979 that increased serum concentrations of 1,25-dihydroxy-vitamin D3 (calcitriol; 1,25(OH)2D3) are associated with the hypercalcaemia in sarcoidosis.17 ,18 Two years later it became clear that the site for overproduction of calcitriol must be extrarenal since hypercalcaemia and raised calcitriol levels were observed in an anephric patient with sarcoidosis.19 The puzzle was finally solved in 1983 with the report that cultured alveolar macrophages in sarcoidosis are able to produce calcitriol.20
Epidemiology
Bone involvement is reported to be from 1% to 34% depending on the primary interest of the author and whether a radiological evaluation of the bones has been performed,21 though the recognition of this problem has increased since the introduction of computed tomographic (CT) scanning. In an untreated group of patients we have found that, when sarcoidosis was known for at least 20 months, vertebral cancellous mineral content was lower than normal (>1 SD below normal—that is, Z score < –1) in seven of 14 men, in four of six young women, and in three of five postmenopausal women. Thus, over 50% of patients with chronic sarcoidosis had osteopenia.22
Hypercalcaemia (above 11 mg/dl or above 0.11 kg/m3) occurs in less than 10% and clinically important hypercalcaemia probably occurs in less than 5% of patients with sarcoidosis.23 Hypercalciuria is found more frequently. Taking an upper limit of urinary calcium excretion rate of 300 mg/24 hours, it was found in 77 (40%) of 192 patients in London.24 Renal calculi have been found in about 10% of patients with chronic sarcoidosis, with a prevalence ranging from 1.3% to 14%.25-30 In rare cases (2.2% in one retrospective study, 3.6% in one prospective study) they may be the presenting feature of the disease.31 ,32 Moreover, there may be asymptomatic renal stones at presentation in a further 2.7%.32
Pathogenesis of extrarenal synthesis of 1,25(OH)2D3: a compensatory mechanism mounted by the immune system?
The structure of the 1,25(OH)2D3 that was synthesised by the sarcoid alveolar macrophages was confirmed by mass spectroanalysis.33 Production of 1,25(OH)2D3 in the system was enhanced in a dose dependent fashion by γ-interferon.34 ,35 γ-Interferon is produced spontaneously by activated lymphocytes and alveolar macrophages in active sarcoidosis.36 These findings provide evidence that γ-interferon plays a major role in the pathogenesis of extrarenal synthesis of 1,25(OH)2D3.
Alveolar macrophages recovered by bronchoalveolar lavage from patients with sarcoidosis possess 1α-hydroxylase activity and are able to metabolise 1,25(OH)2D3 from 25-hydroxy-vitamin D3.20 Substrate specificity and enzyme affinity for 25-hydroxy-vitamin D3 are similar to those reported for the renal enzyme.34 Whereas synthesis of 1,25(OH)2D3 by the pulmonary alveolar macrophages and mammalian kidney show some similarities, 25(OH)D-1α-hydroxylase from the sarcoid macrophages differs from the renal enzyme in a number of important respects. In contrast to renal 25(OH)D-24-hydroxylase, 25(OH)D-24-hydroxylase in the alveolar macrophage is stimulated only at very high concentrations of 1,25(OH)2D3.35 Unlike mammalian renal cells,37-41 little inhibition of 25(OH)D-1α-hydroxylase activity occurs in response to 1,25(OH)2D3 in pulmonary alveolar macrophages.35 Synthesis of the metabolite is markedly diminished by the addition of dexamethasone directly to the in vitro system, and inhibition is dose dependent.34 ,35These in vitro studies help to account for the clinical observations that serum 1,25(OH)2D3 in patients with sarcoidosis is not well regulated and is reduced by glucocorticoids.17 ,19 ,42
Receptors for 1,25(OH)2D3 are present in activated peripheral T lymphocytes from normal human subjects.431,25(OH)2D3 was shown to inhibit the proliferation of T cells and to suppress interleukin-2 activity44 and γ-interferon synthesis45 by phytohaemagglutinin stimulated human peripheral lymphocytes. 1,25(OH)2D3 was found to inhibit activated T helper lymphocyte activity from normal human subjects in vitro.46 If receptors for 1,25(OH)2D3 are present in activated pulmonary lymphocytes and if 1,25(OH)2D3 inhibits the production of γ-interferon and the proliferation of activated T cells in granulomas of patients with sarcoidosis, production of 1,25(OH)2D3 by alveolar macrophages could provide a compensatory mechanism mounted by the immune system to inhibit the inflammatory process.47 ,48 In other words, 1,25(OH)2D3 may be an important downregulator of the intensity of the T lymphocyte activity at sites of disease activity by its ability to limit T helper cell proliferation and to inhibit lymphokine production from these cells.
Pathogenesis of abnormal calcium metabolism
Regardless of the potential role of 1,25(OH)2D3 in the modulation of inflammation, it is evident that granulomas provide a non-renal source of 1,25(OH)2D3. This has been demonstrated in diseased lymph nodes49 and in alveolar macrophages.50 This hyperproduction may result in enhanced intestinal absorption of calcium, as shown by balance studies and measurement of calcium absorption with radiolabelled calcium.51-54 Consequently hypercalcaemia, hypercalciuria, nephrocalcinosis and renal stones may occur, while serum immunoreactive parathyroid hormone is either suppressed or in the low to normal range.17-19 Hypercalcaemia usually develops only when the calcium burden coming from the increased intestinal absorption is very high, or when there is some degree of renal insufficiency.18 Hypercalcaemia varies directly with calcium intake52 ,53 and can be prevented or corrected by dietary restriction of calcium. Exposure to sunlight or to ultraviolet light may be deleterious because of the induction of skin overproduction of vitamin D3.47 For the same reason a seasonal incidence of hypercalcaemia may be seen in summer in patients with sarcoidosis.23
The story, however, is not so simple because increases in urinary hydroxyproline levels, an index of bone resorption, occur in sarcoidosis55 which means that some of the excess urinary calcium may originate from the skeleton. In addition, high levels of 1,25(OH)2D3 may stimulate osteoclastic activity and bone resorption.50-58
Clinical impact
Hypercalcaemia and hypercalciuria are usually asymptomatic but the toxic effects of calcium on renal tubules may produce symptoms of polyuria, volume depletion, and polydipsia.26 ,59Nephrogenic diabetes insipidus and other tubular defects (wasting of potassium, magnesium, phosphate, glucose and amino acids, metabolic acidosis or alkalosis) are described,59 but their occurrence is very rare. Depending on its duration and severity, hypercalcaemia may lead, rarely, to acute renal failure, or more frequently to chronic changes in interstitial calcium deposition, and interstitial fibrosis with possible chronic renal insufficiency. Acute hypercalcaemia may result in renal tubule necrosis from intracellular calcium overload and tubule obstruction by calcium precipitates. Nephrocalcinosis occurs in fewer than 5% of patients with sarcoidosis but in more than 50% of patients with renal insufficiency,26 and is the major cause of chronic renal failure in sarcoidosis.59 It is found more often in renal biopsy samples or at necropsy than in radiographs. Renal calculi have already been described in this report (see above). Nephrolithiasis may in turn impair renal function by obstructing the urinary tract with resulting hydronephrosis and need for invasive procedures such as lithotripsy, endoscopic treatment, percutaneous intervention or surgical removal.
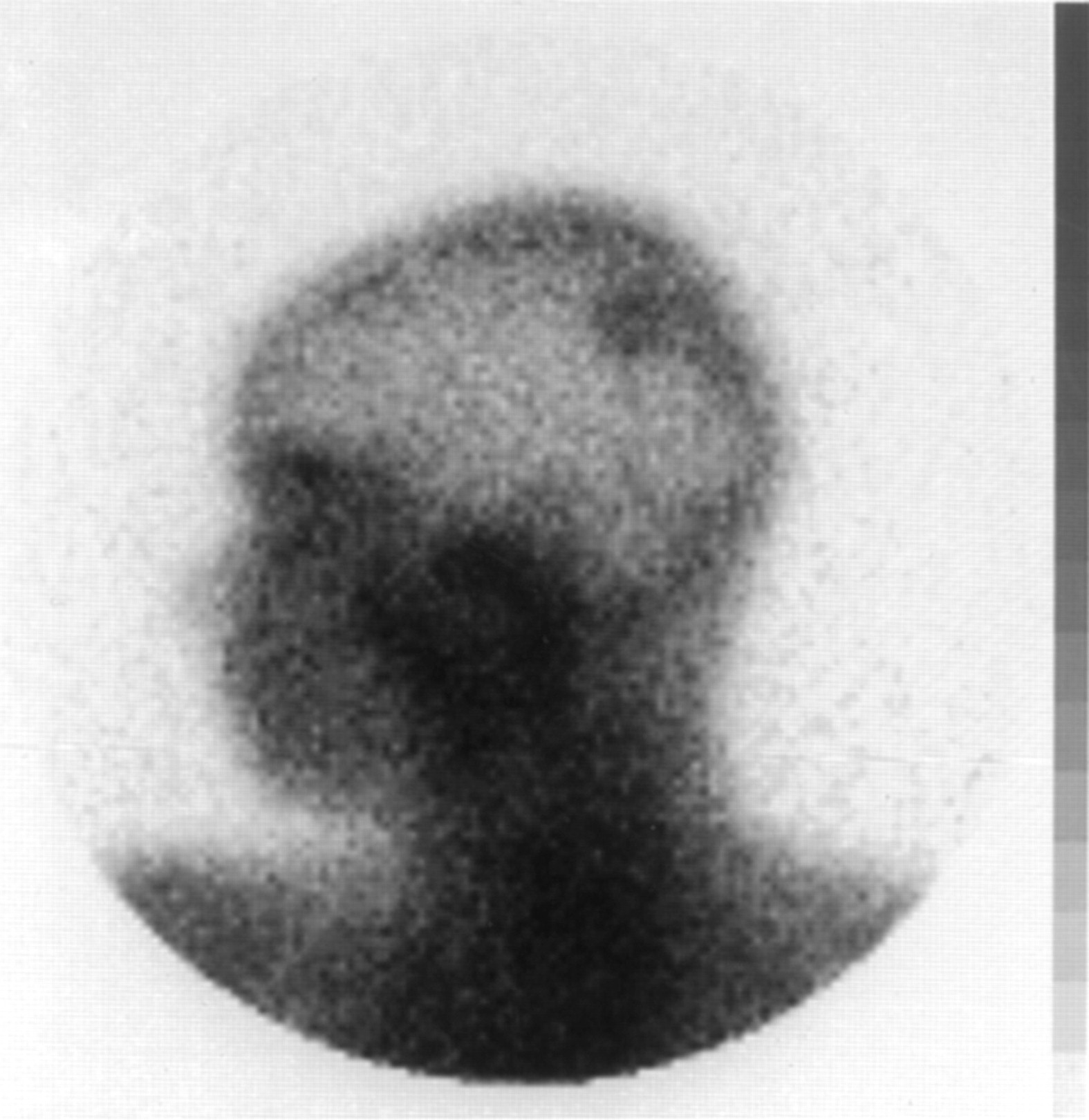
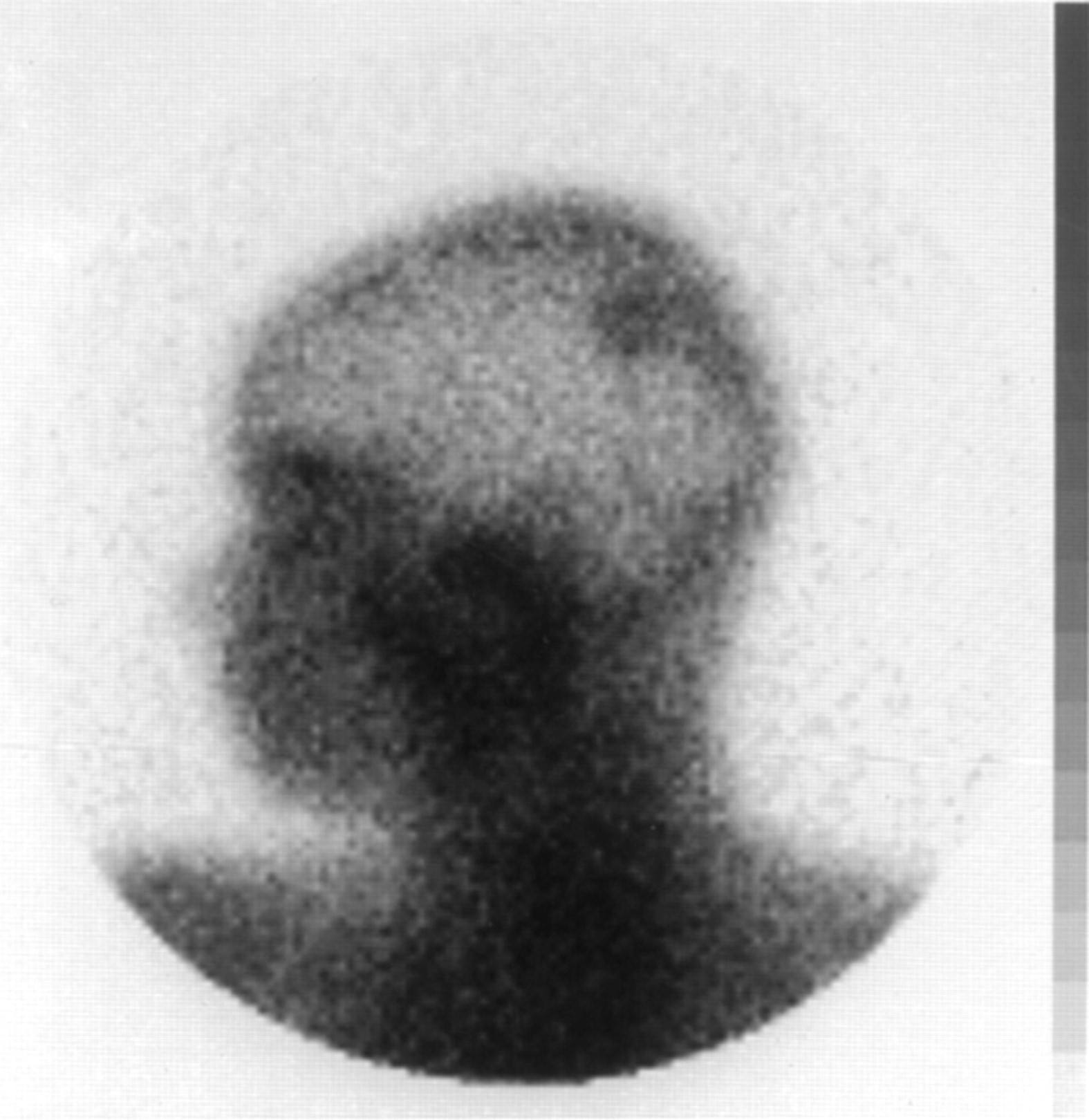
Radiological evaluation of the skeleton is not included in the work up of the disease as presented in the ATS/ERS/WASOG guidelines at the last Congress of the World Association for Sarcoidosis and Other Granulomatous Disorders held in Essen, Germany in September 1997. Nevertheless, it may show that the small bones of the hands and feet are affected frequently, especially the middle and distal phalanges.60 Scattered osteosclerotic changes may also be noted in the skull, long bones, ribs or elsewhere, and may be an occasional finding of a total body scan with gallium-67 (fig 1). Cyst-like lesions of various sizes may also be present occasionally. However, skeletal involvement may be assessed best by bone scintigraphy.61
{kind=link}
Total body scan with gallium-67 showing uptake due to an asymptomatic (and unsuspected) sarcoid bone lesion of the skull.
Treatment
Hypercalcaemia, hypercalciuria and calcaemic nephropathy may be prevented by a low calcium diet, adequate hydration, and minimisation of exposure to light. Milk, cheese, calcium-containing antacids, and vitamin D should be avoided. Corticosteroids are the mainstay of treatment for more severe hypercalcaemia occurring despite these preventive measures. They block extrarenal synthesis of calcitriol by directly inhibiting macrophage 1α-hydroxylase activity and by suppressing the immune activation of macrophages. In relatively low doses (10–20 mg/day) prednisone is rapidly effective in correcting hypercalcaemia; renal function will be corrected to the extent permitted by any irreversible renal damage that has occurred.
The time honoured advice to eat a diet low in calcium has been extended to most non-sarcoidosis patients with kidney stones. Curhanet al 62 have recently reported the results of a prospective epidemiological study of patients with kidney stones from any cause. The incidence of new kidney stones during a four year follow up was lower by almost 50% in men with the highest calcium intake. The authors suggest reasonably, but without direct supporting data, that this unexpected observation may reflect the effect of increased dietary intake of calcium in precipitating oxalate in the gut, thereby reducing intestinal absorption and urinary excretion of oxalate. How this finding may be applied to sarcoidosis is unknown. In our experience most of the renal stones in patients with sarcoidosis are of calcium oxalate. We advise patients to drink sufficient water to keep the urine volume above two litres per day, and, when oxaluria is above 40 mg/24 hours, to limit their intake of oxalate-rich foods (nuts, pepper, chocolate, dark green vegetables, tomato and fruit).63
Long term corticosteroid therapy may be needed in sarcoidosis for many different reasons. In such cases osteopenia is very frequent and occurs in up to 70% of patients when CT scanning is used.14 In sarcoidosis the preventive therapy with calcium or vitamin D may be contraindicated so that the options are not so many; however, osteopenia may be reduced in different ways. In a prospective study on chronic patients needing long term corticosteroid therapy we have shown that bone loss and fractures were lower when using deflazacort compared with prednisone,64 but the study was not double blind and other studies are needed to confirm such a result. In another study we have shown that salmon calcitonin may be a good tool for preventing corticosteroid induced osteoporosis in patients with sarcoidosis.65 Our results with calcitonin were confirmed in a group of 103 patients (four with sarcoidosis) needing long term corticosteroid therapy.66 Bisphosphonates are also good antiresorptive agents and thus are useful for preventing67 or treating68corticosteroid-induced osteoporosis. Only one study is underway on the use of alendronate in patients with sarcoidosis and the preliminary results, which are good, were presented at the recent WASOG Congress held in Essen in September 1997.69 Oral calcium may be given to patients without hypercalciuria, but calciuria needs careful monitoring in this case. It is clear that we do not have to accept bone loss and high fracture rates as inevitable consequences of high dose glucocorticoid therapy. The challenge now is to make the assessment of the risk of osteoporosis an integral part of the decision to commence glucocorticoid therapy so that treatment may be introduced before fractures occur. Such a practice will avert substantial iatrogenic morbidity in this already disabled group of patients.70
For the rare patient who cannot be given corticosteroids there are two other therapeutic options for hypercalcaemia: chloroquine and ketaconazole. Both are inhibitors of 1α-hydroxylase. Chloroquine and hydroxychloroquine71 ,72 have potential retinal toxicity which may limit their use, but this is not the case if the dosage is limited to 250 mg/day. At higher doses a close ophthalmological follow up is suggested in the long term. Ketaconazole has been given in a dose of 800 mg/day for two years to a 47 year old patient with hypercalcaemia with a good result (but with some decrease in serum testosterone levels and libido).73 Two other reports are less favourable because, using the same dosage, renal function deteriorated in two patients after four to six days of treatment74 and in one patient the drug had to be discontinued after four months because of hepatotoxic side effects.75 Oral phosphates are another therapeutic option because they limit intestinal calcium absorption.76
Diuretics may increase or decrease the calcium concentration in plasma and urine depending on the type of diuretic employed.77 Thiazide diuretics (hydrochlorothiazide, chlortalidone) decrease the renal excretion of Ca++ as a result of a direct action on the early distal tubule, thereby increasing calcaemia. They are contraindicated if the patient has hypercalcaemia, but may be an option to decrease hypercalciuria in normocalcaemic patients if the serum calcium levels are carefully monitored.
Whether or not hypercalciuria unaccompanied by hypercalcaemia or renal stones requires treatment is, however, an open question. Lebacqet al 78 have suggested administration of 5 g cellulose phosphate daily by mouth, or hydrochlorothiazide in a dose of 100 mg daily. Amiloride also decreases excretion of Ca++.77 Our practice in the Milan Sarcoid Clinic is to give to such patients a calciuria decreasing diuretic when two consecutive determinations of 24 hour calciuria are over 500 mg in spite of a low calcium diet. However, in spite of the rational basis, this practice remains poorly investigated and prospective studies are needed.
In contrast, loop diuretics (furosemide) enhance the excretion of Ca++. The calciuric action of these agents is the basis for their use in symptomatic hypercalcaemia. Spironolactone also increases Ca++ excretion through a direct effect on tubular transport.